You might also like
- NCP-Acute Postpartum Perineal PainDocument2 pagesNCP-Acute Postpartum Perineal PainFrenzylane Diane CoralNo ratings yet
- All Art Is Propaganda PDFDocument2,708 pagesAll Art Is Propaganda PDFPau_Brand_255033% (3)
- Calculus Cheat Sheet DerivativesDocument4 pagesCalculus Cheat Sheet DerivativesRajatNo ratings yet
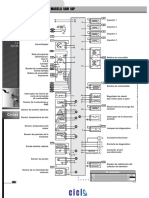
- Renault Inyección Electrónica Kangoo RL-RN 1.6 1999 Siemens Sirius 32b PDFDocument2 pagesRenault Inyección Electrónica Kangoo RL-RN 1.6 1999 Siemens Sirius 32b PDFOsvaldo LópezNo ratings yet
- Taita Salasaca - Conga Drums 2Document2 pagesTaita Salasaca - Conga Drums 2Carlos XavierNo ratings yet
- 6periostitisDocument10 pages6periostitisAntonioNo ratings yet
- 5756867Document1,027 pages5756867Sách Việt Nam50% (2)
- GM Relés y Fusibles Corsa PDFDocument1 pageGM Relés y Fusibles Corsa PDFcorylinNo ratings yet
- Ibfc 142 Engenheiro MecanicoDocument16 pagesIbfc 142 Engenheiro MecanicoJosé Maria junior100% (2)
- 5Document2 pages5Abel Salazar PianoNo ratings yet
- Strong Enough - DrumsDocument2 pagesStrong Enough - DrumsКолянсур ИвановNo ratings yet
- Extracto Destinos-Elementos-para-la-gestión-de-destinos-turisticosDocument76 pagesExtracto Destinos-Elementos-para-la-gestión-de-destinos-turisticosEnzo Navarrete UlloaNo ratings yet
- Escort 18 16 ZetecDocument2 pagesEscort 18 16 ZetecOsvaldo LópezNo ratings yet
- Los Mareados Arreglo Hernan PossettiDocument2 pagesLos Mareados Arreglo Hernan PossettiteomondejarmusicaNo ratings yet
- UTS ELT MDE S1 Coursebook Evaluation ChecklistDocument3 pagesUTS ELT MDE S1 Coursebook Evaluation ChecklistHanin Khalishah WaqqasNo ratings yet
- PDF Parts Catalog Tvs Rockz - CompressDocument104 pagesPDF Parts Catalog Tvs Rockz - CompressaspareteNo ratings yet
- Cicuta Tibia - TubaDocument2 pagesCicuta Tibia - TubaYohan Octavio Vera DelgadoNo ratings yet
- Ampacidad AlimentacionDocument1 pageAmpacidad Alimentacionluis miguel sanchez estrellaNo ratings yet
- Hecho Del PíncipeDocument11 pagesHecho Del PíncipeEdisson MoralesNo ratings yet
- Building ActDocument136 pagesBuilding ActVeronika RaušováNo ratings yet
- 101 Problems in AlgebraDocument160 pages101 Problems in AlgebraTrishaii Cuaresma96% (28)
- Xsara 18 - Berlingo 18 - 18 Xu7jb PDFDocument2 pagesXsara 18 - Berlingo 18 - 18 Xu7jb PDFJorge Daniel DiazNo ratings yet
- What A Wonderful World Eb - Bass Trombone PDFDocument1 pageWhat A Wonderful World Eb - Bass Trombone PDFJose HerreroNo ratings yet
- All The Things You AreDocument1 pageAll The Things You ArePeppe LiottaNo ratings yet
- Trompeta 1Document2 pagesTrompeta 1Mauricio TorresNo ratings yet
- GM Inyección Electrónica S10 Blazer 2.2 Efi Delphi Multec emDocument2 pagesGM Inyección Electrónica S10 Blazer 2.2 Efi Delphi Multec emyayixdfuego131No ratings yet
- Fiat CoupeDocument1 pageFiat CoupeJulio FaninNo ratings yet
- Greenwashing Nas EmpresasDocument37 pagesGreenwashing Nas EmpresasLara GagoNo ratings yet
- Excercise in FDocument2 pagesExcercise in FPaz Villahoz100% (2)
- 388 1006 1 PBDocument20 pages388 1006 1 PBGabriel Evangelista dos SantosNo ratings yet
- Aural RitmoDocument1 pageAural RitmofabioNo ratings yet
- Como Quien Pierde Una Estrella VozDocument2 pagesComo Quien Pierde Una Estrella VozGerardo100% (2)
- 2020Document14 pages2020mintrikpalougoudjoNo ratings yet
- Renault Inyección Electrónica Clio 1.4 Ac Delco Monopoint P PDFDocument2 pagesRenault Inyección Electrónica Clio 1.4 Ac Delco Monopoint P PDFGood CarNo ratings yet
- Music To Watch Girls by MJDocument3 pagesMusic To Watch Girls by MJMarvin JongNo ratings yet
- Flow Design Formulas For Calculation - Exported From (HTM - 02 - 01 - Part - A)Document8 pagesFlow Design Formulas For Calculation - Exported From (HTM - 02 - 01 - Part - A)wesam allabadi50% (2)
- Planes APIDocument10 pagesPlanes APIManuel FigueroaNo ratings yet
- Paradise Violín IIDocument2 pagesParadise Violín IIJavier Rubio PérezNo ratings yet
- Enfermeiro Ebsrh 2015Document10 pagesEnfermeiro Ebsrh 2015Neila Reis da SilvaNo ratings yet
- Business Startup Guides-Preparing Yourself Ver 2Document4 pagesBusiness Startup Guides-Preparing Yourself Ver 2Minh Huỳnh100% (1)
- Detail (1-1) To R.C. Strip Footing (Sf1) : A B E F H J KDocument1 pageDetail (1-1) To R.C. Strip Footing (Sf1) : A B E F H J KThomas Garcia0% (1)
- Charles D Ghilani - Paul R Wolf - Elementary Surveying - An Introduction To Geomatics-Pearson Prentice Hall (2012) - ExtractoDocument19 pagesCharles D Ghilani - Paul R Wolf - Elementary Surveying - An Introduction To Geomatics-Pearson Prentice Hall (2012) - ExtractoRodrigo DelBarrioNo ratings yet
- 09 - Chapter 1Document20 pages09 - Chapter 1Dr. POONAM KAUSHALNo ratings yet
- Mix Trompeta ChilombianoDocument1 pageMix Trompeta ChilombianoDenise AlvaradoNo ratings yet
- 01 - Lista de Parametros SimplificadaDocument8 pages01 - Lista de Parametros SimplificadaLuis Felipe VidigalNo ratings yet
- Tu Me Gustas Trompeta 1Document2 pagesTu Me Gustas Trompeta 1JonathanNo ratings yet
- ElvisDocument1 pageElvismaui3No ratings yet
- Indian Express 19 AugustDocument20 pagesIndian Express 19 AugustTension Dene kaNo ratings yet
- Elec 4 BlackDocument1 pageElec 4 Blackyudo08No ratings yet
- Trompeta 2Document2 pagesTrompeta 2Mauricio TorresNo ratings yet
- Tema 6. CULTURADocument7 pagesTema 6. CULTURAMarinaNo ratings yet
- El Pastor - VihuelaDocument1 pageEl Pastor - VihuelaDamian Guardia SalazarNo ratings yet
- Lagenda Violin PDFDocument2 pagesLagenda Violin PDFMarvin Jong0% (1)
- Mix Serpiente - BandaDocument53 pagesMix Serpiente - BandaJohn Carlos Vilca VelizNo ratings yet
- LBP - Dr. Dessy Sp.sDocument77 pagesLBP - Dr. Dessy Sp.srahmadsyahNo ratings yet
- Trigeminal Autonomic CephalgiasDocument15 pagesTrigeminal Autonomic Cephalgiasheni taridaNo ratings yet
- KaufmanDocument2 pagesKaufmanrbtakemotoNo ratings yet
- Cancer Pain ManagementDocument22 pagesCancer Pain ManagementWanie Kaflee100% (1)
- Types of PainDocument1 pageTypes of PainIntan Putri Wirahana ShantyNo ratings yet
- Chronic Paroxysmal Hemicrania Neurological-Conditions/chronic-Paroxysmal-Hemicrania)Document2 pagesChronic Paroxysmal Hemicrania Neurological-Conditions/chronic-Paroxysmal-Hemicrania)fitriaNo ratings yet
- Cefalea - Clasificacion de Cefaleas ICHD-IIR1 FinalDocument234 pagesCefalea - Clasificacion de Cefaleas ICHD-IIR1 FinalRaul KimNo ratings yet
- MC KenzieDocument6 pagesMC KenzieYulia DiniNo ratings yet
- Neuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)Document27 pagesNeuraxial Anaesthesia: DR Ali Rahman Assistant Professor - Anaesthesiology Department (RMDC)fahadali2000No ratings yet
- Dry Needling Article SRF JournalDocument3 pagesDry Needling Article SRF JournalObreNo ratings yet
- Daftar Diagnosis Dan Kode BPJSDocument18 pagesDaftar Diagnosis Dan Kode BPJSeginagirsangNo ratings yet
- BASH Guidelines Update 2 - v5 1 Indd PDFDocument53 pagesBASH Guidelines Update 2 - v5 1 Indd PDFnephylymNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaAlmira Shabrina SaraswatiNo ratings yet
- Myofascial PainDocument8 pagesMyofascial PainEnyaw Droffats100% (1)
- Essential Anesthesia From Science To Practice,.46Document1 pageEssential Anesthesia From Science To Practice,.46Jean PaulNo ratings yet
- Dr. Moch. Bahrudin, SP.S: Bagian Neurologi Fakultas Kedokteran Universitas Muhammadiyah MalangDocument34 pagesDr. Moch. Bahrudin, SP.S: Bagian Neurologi Fakultas Kedokteran Universitas Muhammadiyah MalangputrimeilissaNo ratings yet
- Fact Sheet Trigeminal NeuralgiaDocument2 pagesFact Sheet Trigeminal Neuralgiasarmad78No ratings yet
- Tens-Transcutaneous Electrical Nerve StimulationDocument35 pagesTens-Transcutaneous Electrical Nerve Stimulationtamilvanan3100% (2)
- Dry NeedlingDocument11 pagesDry Needlingapi-468018392100% (1)
- Myofascial Trigger Points - Pathophysiology and Evidence-Informed Diagnosis and Management (Contemporary Issues in Physical Therapy and Rehabilitation Medicine) (PDFDrive)Document306 pagesMyofascial Trigger Points - Pathophysiology and Evidence-Informed Diagnosis and Management (Contemporary Issues in Physical Therapy and Rehabilitation Medicine) (PDFDrive)Christine DiVirgilioNo ratings yet
- The International Association For The Study of Pain (IASP) Classification of Chronic Pain Syndromes. Pain, 1101-1103.Document3 pagesThe International Association For The Study of Pain (IASP) Classification of Chronic Pain Syndromes. Pain, 1101-1103.Fran WermannNo ratings yet
- Daftar PustakaDocument6 pagesDaftar Pustakahildaali020No ratings yet
- PT Asuransi Jiwa Inhealth IndonesiaDocument1 pagePT Asuransi Jiwa Inhealth Indonesiabob saragihNo ratings yet
- Pain NotesDocument4 pagesPain Notesrazelgc100% (4)
- Teknik Assesment NyeriDocument20 pagesTeknik Assesment NyerisrininingNo ratings yet
- AnestheticsDocument11 pagesAnestheticsKalidasan KrishnaNo ratings yet
- DD Lumbalgia PDFDocument22 pagesDD Lumbalgia PDFJose Antonio Giron MombielaNo ratings yet
- Value of Transcutaneous Electric Nerve StimulationDocument5 pagesValue of Transcutaneous Electric Nerve StimulationIndah YulantariNo ratings yet
- Cervicogenic Headache Differential DiagnosisDocument10 pagesCervicogenic Headache Differential Diagnosispuchio100% (1)