You might also like
- HSE Report On Mooring IntegrityDocument313 pagesHSE Report On Mooring IntegritysanumajNo ratings yet
- Chronic PainDocument12 pagesChronic PainlizNo ratings yet
- Banaba Tea Aids Weight LossDocument5 pagesBanaba Tea Aids Weight LossAveriAlonzoNo ratings yet
- نسخة Lecture - PAIN Assessment & ManagementDocument52 pagesنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Understanding PainDocument23 pagesUnderstanding Painnisha justinNo ratings yet
- Production Choke BasicsDocument39 pagesProduction Choke Basicsbtmohamed7084100% (1)
- PainDocument35 pagesPainixora n100% (1)
- Conquering Pain: How to Prevent It, Treat It and Lead a Better LifeFrom EverandConquering Pain: How to Prevent It, Treat It and Lead a Better LifeRating: 5 out of 5 stars5/5 (1)
- Company & Project Information for Electrical, Instrumentation ServicesDocument28 pagesCompany & Project Information for Electrical, Instrumentation ServicesMrudul PatilNo ratings yet
- Assessing and Managing Pain: A Guide for NursesDocument58 pagesAssessing and Managing Pain: A Guide for NursesErica GyeolsilNo ratings yet
- Pain Management CHNDocument38 pagesPain Management CHNVaibhavi ShastriNo ratings yet
- Pain Management For NursesDocument42 pagesPain Management For Nursesblacknurse100% (1)
- Acute Pain NCPDocument6 pagesAcute Pain NCPPesky Pescante-MonterolaNo ratings yet
- To Study The Open Circuit/Core Losses of Single Phase TransformerDocument5 pagesTo Study The Open Circuit/Core Losses of Single Phase TransformerTanzeel UR RehmanNo ratings yet
- DR - Muhammad Aasam Maan: Consultant Pain SpecialistDocument23 pagesDR - Muhammad Aasam Maan: Consultant Pain SpecialistMuhammad Aasim MaanNo ratings yet
- Holistic Pain Relief: How to ease muscles, joints and other painful conditionsFrom EverandHolistic Pain Relief: How to ease muscles, joints and other painful conditionsNo ratings yet
- Industrial Attachment at Meghna Knit Composite Ltd.Document137 pagesIndustrial Attachment at Meghna Knit Composite Ltd.Riasat Alam50% (2)
- Acute Service Pain Handbook 2011Document116 pagesAcute Service Pain Handbook 2011Iskandar414No ratings yet
- Siehl, Caitlyn-Whatweburied Digitaledition (2015)Document64 pagesSiehl, Caitlyn-Whatweburied Digitaledition (2015)Bahar Gaser100% (1)
- Journal On PainDocument5 pagesJournal On PainGeevine CansinoNo ratings yet
- Pathophysiology of PainDocument6 pagesPathophysiology of PainJorgeGalleguillosCavadaNo ratings yet
- Basic CourseDocument97 pagesBasic CourseAhmed KhairyNo ratings yet
- Managing Neuropathic PainDocument10 pagesManaging Neuropathic PainAgusBhakti100% (1)
- Unit-3 - Pain ManagementDocument100 pagesUnit-3 - Pain ManagementyaraNo ratings yet
- Topical Meds for Neuropathic Orofacial PainDocument13 pagesTopical Meds for Neuropathic Orofacial PainMarco Antonio Morales OsorioNo ratings yet
- CHAPTER 15 Pain ManagementDocument35 pagesCHAPTER 15 Pain ManagementIfy OhansonNo ratings yet
- Neuralgia Trigeminal-EnglishDocument29 pagesNeuralgia Trigeminal-EnglishUcc Ang BangarenNo ratings yet
- A.M.Takdir MusbaDocument31 pagesA.M.Takdir MusbaarifwahyudiNo ratings yet
- Chronic Facial Pain Guide: Causes, Symptoms & TreatmentsDocument5 pagesChronic Facial Pain Guide: Causes, Symptoms & TreatmentsdamarstationNo ratings yet
- How To Diagnose LBP RevisiDocument65 pagesHow To Diagnose LBP RevisiDedy SavradinataNo ratings yet
- Teaching Student Nurses Effective Pain ManagementDocument18 pagesTeaching Student Nurses Effective Pain ManagementMuhamad GumilangNo ratings yet
- Overview of Neuropathic Pain ManagementDocument32 pagesOverview of Neuropathic Pain ManagementBernad NauliNo ratings yet
- PMT 2018 0061Document4 pagesPMT 2018 0061jose perezNo ratings yet
- Nyeri Akut Dan Kronik: Kuliah 23-24 Maret 2023 U B, Malang PPDS, Koass Dan DR MudaDocument53 pagesNyeri Akut Dan Kronik: Kuliah 23-24 Maret 2023 U B, Malang PPDS, Koass Dan DR MudaDManestesi cokicokiNo ratings yet
- Neuropathies: Essential Oils Show Promising Results in The Fight Against SymptomsDocument17 pagesNeuropathies: Essential Oils Show Promising Results in The Fight Against Symptomskcc2012No ratings yet
- Konsep Nyeri Dan Manajemen NyeriDocument36 pagesKonsep Nyeri Dan Manajemen NyeriFira AlumanNo ratings yet
- Music Intervention For Burn PatientDocument8 pagesMusic Intervention For Burn PatientMedhia IqlimaNo ratings yet
- Jurnal Reading PainDocument36 pagesJurnal Reading PainvindaNo ratings yet
- By Dr. Cuong Ngo-Minh Back To Basics April 14th 2010Document15 pagesBy Dr. Cuong Ngo-Minh Back To Basics April 14th 2010Wael WilsonNo ratings yet
- Pain Management For Medical StudentsDocument37 pagesPain Management For Medical Studentsamq aloqiliNo ratings yet
- Assessing and treating pediatric painDocument11 pagesAssessing and treating pediatric painfuka priesleyNo ratings yet
- PAINDocument41 pagesPAINPrasenjit ChakrabortyNo ratings yet
- Assessment and Treatment of Pain in Pediatric PatientsDocument10 pagesAssessment and Treatment of Pain in Pediatric PatientsAnonymous zd0Bwj4nNo ratings yet
- 8 Chronic Pain ManagementDocument14 pages8 Chronic Pain ManagementEndang Dwi KurniaNo ratings yet
- The PainDocument19 pagesThe PainKevin Torres PonteNo ratings yet
- Chronic Back Pain: Long Case 17Document4 pagesChronic Back Pain: Long Case 17Shujaat Nazir KhanNo ratings yet
- Barriers To Reconceptulization of Chronic Pain Moseley PDFDocument6 pagesBarriers To Reconceptulization of Chronic Pain Moseley PDFpfi_jenNo ratings yet
- PAINDocument11 pagesPAINvavafo7699No ratings yet
- Supplementary Material 7a Analgesia, Sedation and Neuromuscular BlockadeDocument10 pagesSupplementary Material 7a Analgesia, Sedation and Neuromuscular BlockadeJeremiah Andre Poissonier AyupanNo ratings yet
- Materi Pelatihan Manajemen Nyeri 2019Document52 pagesMateri Pelatihan Manajemen Nyeri 2019Iman Muhamad FirmansyahNo ratings yet
- Penatalaksanaan Nyeri: Dr. Pangkuwidjaja P Departemen Anestesiologi Fakultas Kedokteran Unika Atma JayaDocument40 pagesPenatalaksanaan Nyeri: Dr. Pangkuwidjaja P Departemen Anestesiologi Fakultas Kedokteran Unika Atma JayaalbertlimNo ratings yet
- Pain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalDocument50 pagesPain Management in The Emergency: Dr. Prathiba Prasad Emergency Physician Masafi HospitalPrathiba PrassaddNo ratings yet
- Cavite State University Module on Pathophysiology of PainDocument14 pagesCavite State University Module on Pathophysiology of PainDennis Nyambane MomanyiNo ratings yet
- Trigeminal NeuralgiaDocument37 pagesTrigeminal Neuralgiawahyu purnamaNo ratings yet
- Chapter 005Document4 pagesChapter 005Natalia Page TrevinoNo ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- Pathway For Pain Perception and Response: What Is ??Document6 pagesPathway For Pain Perception and Response: What Is ??Jc MendiolaNo ratings yet
- Competency Appraisal 2: Pain ManagementDocument96 pagesCompetency Appraisal 2: Pain ManagementLane Mae Magpatoc NoerrotNo ratings yet
- HHS Public Access: Demystifying Post-Stroke Pain: From Etiology To TreatmentDocument21 pagesHHS Public Access: Demystifying Post-Stroke Pain: From Etiology To TreatmentMartha OktaviaNo ratings yet
- Pain Management in Children: Pediatric AssignmentDocument5 pagesPain Management in Children: Pediatric AssignmentAbdulbari AL-GhamdiNo ratings yet
- PainDocument36 pagesPainabhijithr1817No ratings yet
- Neuropathic Pain: Definition, Assessment and Epidemiology: SciencedirectDocument10 pagesNeuropathic Pain: Definition, Assessment and Epidemiology: SciencedirectLidwina ApyakaNo ratings yet
- Pain AssessmentDocument12 pagesPain AssessmentFadhilah Asyifa DewantiNo ratings yet
- Lewis Medical-Surgical Nursing Chapter 8 Pain Key PointsDocument7 pagesLewis Medical-Surgical Nursing Chapter 8 Pain Key PointsAmber Nicole HubbardNo ratings yet
- Trigeminal Neuralgia: Defination: According To Iasp (International Association For The Study of Pain)Document11 pagesTrigeminal Neuralgia: Defination: According To Iasp (International Association For The Study of Pain)saketaggarwalNo ratings yet
- Veterinary Pain ManagementDocument8 pagesVeterinary Pain ManagementMenaNo ratings yet
- EPM Partic Manual 2e FinalDocument64 pagesEPM Partic Manual 2e FinalRyan GusnaintinNo ratings yet
- Fast Facts: Perioperative Pain: Effective management has numerous benefitsFrom EverandFast Facts: Perioperative Pain: Effective management has numerous benefitsNo ratings yet
- Managing Exercise for Developmental Delay ChildrenDocument11 pagesManaging Exercise for Developmental Delay ChildrenDhiya Uddin RNo ratings yet
- 669 2068 1 PBDocument10 pages669 2068 1 PBFicky HaryudiNo ratings yet
- Naskah PublikasiDocument15 pagesNaskah PublikasiMaria Monica Aggi MutiarasariNo ratings yet
- Jurnal Tisa JANTUNG Revisi 3Document12 pagesJurnal Tisa JANTUNG Revisi 3rahmadsyahNo ratings yet
- Katalog Buku Fisioterapi PDFDocument25 pagesKatalog Buku Fisioterapi PDFrachmad100% (1)
- Budget-of-Work-General Biology 1Document2 pagesBudget-of-Work-General Biology 1joei ArqueroNo ratings yet
- 1 PB PDFDocument11 pages1 PB PDFaldo surya pratamaNo ratings yet
- CIA Patho 1Document23 pagesCIA Patho 1Suhas H GNo ratings yet
- Special Report 205 Chemical Weekly 1 4-B PDFDocument7 pagesSpecial Report 205 Chemical Weekly 1 4-B PDFsifrmoroNo ratings yet
- Your Msa Scba System: Cleaning/DisinfectingDocument1 pageYour Msa Scba System: Cleaning/Disinfectingjohn rajNo ratings yet
- Ece-Research Work 1Document10 pagesEce-Research Work 1Peale ObiedoNo ratings yet
- To 1 SMPN 210 JKT Tahun 2016-2017Document11 pagesTo 1 SMPN 210 JKT Tahun 2016-2017Sugeng Supoyo Pawit DigdotriratnaNo ratings yet
- EC538 LTspice IntroDocument10 pagesEC538 LTspice IntroTeferi LemmaNo ratings yet
- ISO Standards in ProcessDocument20 pagesISO Standards in ProcessYeni OktaviaNo ratings yet
- SI 410 Weighing Indicator User ManualDocument64 pagesSI 410 Weighing Indicator User ManualShehab100% (2)
- DPS Nashik Class 12 Science SyllabusDocument18 pagesDPS Nashik Class 12 Science SyllabusSayali Morwal-KumawatNo ratings yet
- Water Cycle Cer 002Document2 pagesWater Cycle Cer 002api-434008934No ratings yet
- Philosophy, Logic, & Rhetoric SyllabusDocument3 pagesPhilosophy, Logic, & Rhetoric SyllabusBrynja KnappNo ratings yet
- Upper Gastro Intestinal BleedingDocument13 pagesUpper Gastro Intestinal BleedingmuniningmicanNo ratings yet
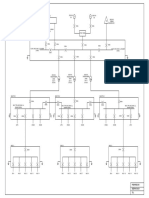
- Conceptual SLDDocument1 pageConceptual SLDakhilNo ratings yet
- 00 - Orientation LessonDocument32 pages00 - Orientation LessonRekha ShahNo ratings yet
- Bushings BrochureDocument14 pagesBushings Brochurebpd21No ratings yet
- Decline of Controversy and the Catholic ChurchDocument3 pagesDecline of Controversy and the Catholic ChurchEugenio PalandriNo ratings yet
- Fault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)Document5 pagesFault Codes: Brake (DSC/DXC (Dynamic Stability Control) - Bosch 8.0 - Tyre Pressure Monitoring)zacarias NiquiceNo ratings yet
- Energy Conversion and Management: Gvidonas Labeckas, Stasys Slavinskas, Irena KanapkieneDocument25 pagesEnergy Conversion and Management: Gvidonas Labeckas, Stasys Slavinskas, Irena KanapkieneVỵ ĐặngNo ratings yet
- A ETHICS-101 Activity-3Document3 pagesA ETHICS-101 Activity-3Liz FuentesNo ratings yet
- Detection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian LynxDocument5 pagesDetection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian Lynxsusey madelit apaza mamaniNo ratings yet