You might also like
- Iso 20395Document51 pagesIso 20395Gilberto NodarseNo ratings yet
- Plus Plastic Tubes Wallchart Tubeguide VS5229Document1 pagePlus Plastic Tubes Wallchart Tubeguide VS5229Gabrielle Diaz50% (2)
- Microbiology PosterDocument1 pageMicrobiology Posterapi-577806584No ratings yet
- Pneumonia - PhysiopediaDocument5 pagesPneumonia - PhysiopediaudesaoilmillNo ratings yet
- Premalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Document60 pagesPremalignant Lesions and Conditions: Submitted by-BALJEET KAUR B.D.S.-3 Year Roll No.15Rajat NangiaNo ratings yet
- CRANIAL Nerves - ExaminationDocument14 pagesCRANIAL Nerves - ExaminationMoussa FarhatNo ratings yet
- Pathology Mcq's - XenoMEDDocument11 pagesPathology Mcq's - XenoMEDfreeuser3No ratings yet
- Edexcel A2 IAL Biology: Topic 6 - Immunity, Infection and ForensicsDocument22 pagesEdexcel A2 IAL Biology: Topic 6 - Immunity, Infection and ForensicsErin100% (4)
- Laboratory Diagnosis of Viral InfectionDocument35 pagesLaboratory Diagnosis of Viral InfectionHairul Anuar83% (18)
- Clinical Molecular Diagnostic Techniques: A Brief ReviewDocument19 pagesClinical Molecular Diagnostic Techniques: A Brief ReviewSorin LazarNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Rheumatoid ArthritisDocument29 pagesRheumatoid ArthritisTamim IshtiaqueNo ratings yet
- Rheumatoid Arthritis: Polyarthritis As Its Most Common Feature. in Addition, Other Tissues May Be DamagedDocument8 pagesRheumatoid Arthritis: Polyarthritis As Its Most Common Feature. in Addition, Other Tissues May Be Damagedحنين حسن عبد علي حسينNo ratings yet
- Acute Fluid Management of Large Burns Pathophysiology, Monitoring, and ResuscitationDocument9 pagesAcute Fluid Management of Large Burns Pathophysiology, Monitoring, and ResuscitationEduardo Espin LanzNo ratings yet
- Lab Diagnosis of Enteric FeverDocument7 pagesLab Diagnosis of Enteric Feverঅর্ণব কোলেNo ratings yet
- Tuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalDocument58 pagesTuberculosis: Dr.V. Gangadharan Professor & Hod Department of Respiratory Medicine Saveetha Medical College HospitalJoanna RachelNo ratings yet
- EmbolismDocument13 pagesEmbolismSandeep Bansal100% (1)
- Diabetes NotesDocument10 pagesDiabetes Notestripj33No ratings yet
- PericarditisDocument3 pagesPericarditisKhalid Mahmud Arifin0% (1)
- Rheumatoid ArthritisDocument38 pagesRheumatoid ArthritisOlga GoryachevaNo ratings yet
- Respiratory SystemDocument41 pagesRespiratory SystemNikkiAbbaNiColeCartagenaNo ratings yet
- Immunological Lab Diagnosis of TuberculosisDocument38 pagesImmunological Lab Diagnosis of TuberculosisRasha EmadNo ratings yet
- Referensi Dari Internet: OverviewDocument7 pagesReferensi Dari Internet: OverviewdantevermillionNo ratings yet
- Acute Lymphoblastic Leukemia (ALL)Document14 pagesAcute Lymphoblastic Leukemia (ALL)Med PhuongNo ratings yet
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Basic Immunology Introduction:: Hypersensitivity ReactionsDocument10 pagesBasic Immunology Introduction:: Hypersensitivity ReactionsRashed ShatnawiNo ratings yet
- Rhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020Document19 pagesRhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020shewo.pirtamNo ratings yet
- Exam Technique, HNBreast, Thyroid&AbdomenDocument9 pagesExam Technique, HNBreast, Thyroid&AbdomenInsyirah Hatta100% (1)
- Module 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - ClementeDocument27 pagesModule 5A: Dental Management of Patients With Asthma: Prepared By: Dr. Maria Luisa Ramos - Clementeelaine100% (1)
- CPC For Students 2016Document10 pagesCPC For Students 2016Kwadwo Sarpong JnrNo ratings yet
- Perioperative AnaphylaxisDocument23 pagesPerioperative AnaphylaxiscrackernetNo ratings yet
- Case Report Rheumatoid ArthritisDocument29 pagesCase Report Rheumatoid ArthritisEmmy Safitri Abbas0% (1)
- MCQs 1Document33 pagesMCQs 1Subrahmanyam SudiNo ratings yet
- Rheumatoid Arthritis "An Autoimmune Mystery"Document23 pagesRheumatoid Arthritis "An Autoimmune Mystery"Manisanthosh KumarNo ratings yet
- Gangrene PowerpointDocument45 pagesGangrene PowerpointAsep DaniNo ratings yet
- Pleural DiseasesDocument52 pagesPleural DiseasesAmolkumar W DiwanNo ratings yet
- Acute Dyspnea First RevisionDocument56 pagesAcute Dyspnea First RevisionAradhanaRamchandaniNo ratings yet
- Anti Hypertensive Drugs - ACE InhibitorDocument16 pagesAnti Hypertensive Drugs - ACE InhibitorApurba Sarker Apu100% (1)
- Sepsis Power Point Slide Presentation - The Guidelines - Implementation For The FutureDocument25 pagesSepsis Power Point Slide Presentation - The Guidelines - Implementation For The Futuremontie13No ratings yet
- Vena Cava Superior SyndromeDocument12 pagesVena Cava Superior SyndromeAgnes SetiawanNo ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Inflamatory Process 5.5.2Document7 pagesInflamatory Process 5.5.2Maxwell C Jay KafwaniNo ratings yet
- Oral Manifestations of Hematological DisordersDocument6 pagesOral Manifestations of Hematological DisordersPoem AroraNo ratings yet
- Acute Lymphoid LeukemiaDocument41 pagesAcute Lymphoid Leukemiaummi ulfahNo ratings yet
- Compartment Syndrome: Sebelas Maret UniversityDocument8 pagesCompartment Syndrome: Sebelas Maret Universitykhrisna satyaksaNo ratings yet
- Gene Therapy For CancerDocument7 pagesGene Therapy For Canceresraa elsharkawyNo ratings yet
- CellulitisDocument18 pagesCellulitismuthia saniNo ratings yet
- UTIDocument17 pagesUTIBongkotchakorn Mind PhonchaiNo ratings yet
- Carcinogenic AgentsDocument32 pagesCarcinogenic AgentsArijit Guha100% (1)
- Hematuria in ChildrenDocument26 pagesHematuria in ChildrenNovenZefanya100% (1)
- By: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar KristineDocument41 pagesBy: Calaour, Carrey Dasco, Danica Amor Dimatulac, Kevin Lim, Shiela Marie Pagulayan, Sheena May Pua, Mar Kristineceudmd3d100% (2)
- Chapter 1. History and Physical Examination - Art and ScienceDocument3 pagesChapter 1. History and Physical Examination - Art and SciencecarolineNo ratings yet
- Rheumatoid ArthritisDocument19 pagesRheumatoid ArthritisLiya AnjelinaNo ratings yet
- Nephrotic and Nephritic Syndrome - 2008Document65 pagesNephrotic and Nephritic Syndrome - 2008rikasusanti101001201No ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Exercise 1Document4 pagesExercise 1azkha_knowles3279No ratings yet
- History Taking2Document25 pagesHistory Taking2Capture UnseenNo ratings yet
- TLS FinalDocument69 pagesTLS FinalGrace Arthur100% (1)
- National Program of Cancer Registries Education and Training SeriesDocument93 pagesNational Program of Cancer Registries Education and Training SeriesNADEEMNo ratings yet
- Imuune Thrombocytopenia (Itp)Document34 pagesImuune Thrombocytopenia (Itp)Roshandiep GillNo ratings yet
- What Is Rheumatoid ArthritisDocument16 pagesWhat Is Rheumatoid ArthritisDurge Raj GhalanNo ratings yet
- Inflammatory Bowel Disease: DefinitionDocument4 pagesInflammatory Bowel Disease: Definitionkarl abiaadNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Surgical Operation Theater StandardsDocument31 pagesSurgical Operation Theater Standardstummalapalli venkateswara raoNo ratings yet
- Screening For MRSA by Dr.T.V.Rao MDDocument30 pagesScreening For MRSA by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Influenza Teaching Current Update 2023 by Dr.T.V.Rao MDDocument100 pagesInfluenza Teaching Current Update 2023 by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- MDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDDocument2 pagesMDR - TB Emerging Methods in Diagnosis Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Artificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDDocument34 pagesArtificial Intelligence in Healthcare Legal and Ethical Considerations Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDocument28 pagesElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Infection Control in Burns PatietnsDocument41 pagesInfection Control in Burns Patietnstummalapalli venkateswara raoNo ratings yet
- Need For Clinical Microbiologists by Dr.T.V.Rao MDDocument2 pagesNeed For Clinical Microbiologists by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- INFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDDocument25 pagesINFECTION CONTROL TRENDS OF CHANGE by Dr.T.V.Rao MDtummalapalli venkateswara rao100% (1)
- MDR-TB An Update by Dr.T.V.Rao MDDocument43 pagesMDR-TB An Update by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- GRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDDocument2 pagesGRAM STAINING AND CLINICAL UTILITY by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Who Is Killing Modern Medicine in IndiaDocument3 pagesWho Is Killing Modern Medicine in Indiatummalapalli venkateswara raoNo ratings yet
- MALDI-ToF in Clinical MicrobiologyDocument39 pagesMALDI-ToF in Clinical Microbiologytummalapalli venkateswara rao100% (1)
- Health Care Associated Infections Creating Drug Resistance AtlasDocument46 pagesHealth Care Associated Infections Creating Drug Resistance Atlastummalapalli venkateswara raoNo ratings yet
- MDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDDocument33 pagesMDR - TB FACTS AND CONCERNS BY Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Auditing Hospital Associated InfectionsDocument59 pagesAuditing Hospital Associated Infectionstummalapalli venkateswara raoNo ratings yet
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 pagesHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- ZIKA VIRUS INFECTION Emerging Public Health ConcernDocument36 pagesZIKA VIRUS INFECTION Emerging Public Health Concerntummalapalli venkateswara rao100% (1)
- AUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDDocument55 pagesAUDITING ANTIBIOGRAMS by Dr.T.V.RaoMDtummalapalli venkateswara rao100% (1)
- INFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDDocument48 pagesINFECTIONS IN DIALYSIS PATIENTS Basis & Prevention by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Surgical Gloves in Health CareDocument29 pagesSurgical Gloves in Health Caretummalapalli venkateswara raoNo ratings yet
- Medical Microbiology in Crisis in IndiaDocument4 pagesMedical Microbiology in Crisis in Indiatummalapalli venkateswara raoNo ratings yet
- Revisiting Blood CulturingDocument2 pagesRevisiting Blood Culturingtummalapalli venkateswara raoNo ratings yet
- Diversity Analysis in Arachis Subspecies Using Phenotypic Characterization and Microsatellite (SSR) MarkersDocument9 pagesDiversity Analysis in Arachis Subspecies Using Phenotypic Characterization and Microsatellite (SSR) Markersbela OktarindaNo ratings yet
- Product BrochureDocument19 pagesProduct BrochureMohamed ChahmiNo ratings yet
- Lab-On-A-Chip Technology: The Future of Point-Of-Care Diagnostic AbilityDocument3 pagesLab-On-A-Chip Technology: The Future of Point-Of-Care Diagnostic Abilityvicente_ortiz_007No ratings yet
- 2012 RI Prelim Bio H2 P3 - With AnswersDocument16 pages2012 RI Prelim Bio H2 P3 - With Answers遠坂凛No ratings yet
- PDFDocument1,029 pagesPDFCk CkNo ratings yet
- BQ - CC - BishopDocument44 pagesBQ - CC - BishopAn K.No ratings yet
- Molecular Biology Lab - Report تقرير عن معمل بيولوجيا جزيئيةDocument19 pagesMolecular Biology Lab - Report تقرير عن معمل بيولوجيا جزيئيةManal AL-KhouliNo ratings yet
- Isolation of Intact Sub-Dermal Secretory Cavities From EucalyptusDocument11 pagesIsolation of Intact Sub-Dermal Secretory Cavities From EucalyptusManoakiNo ratings yet
- MTPC 140: Molecular Biology and DiagnosticsDocument37 pagesMTPC 140: Molecular Biology and DiagnosticsValdez Francis ZaccheauNo ratings yet
- DNeasy Plant HandbookDocument58 pagesDNeasy Plant HandbookilmanhasifiNo ratings yet
- IDEXX Webinar - Dr. Bill Saxon 31-08-2023Document35 pagesIDEXX Webinar - Dr. Bill Saxon 31-08-2023Estefania MoralesNo ratings yet
- National Guidelines For: HIV-1 Viral Load Laboratory TestingDocument86 pagesNational Guidelines For: HIV-1 Viral Load Laboratory TestingVINOD GUPTANo ratings yet
- Genetic EngineeringDocument17 pagesGenetic EngineeringBobbyNo ratings yet
- Biotechnology - Principles and Processes - CompressedDocument113 pagesBiotechnology - Principles and Processes - CompressedPOT SONGNo ratings yet
- Microbial Detection Total Solution: MGI Sequencing Platform For Pathogen Fast IdentificationDocument20 pagesMicrobial Detection Total Solution: MGI Sequencing Platform For Pathogen Fast IdentificationEntio BaezNo ratings yet
- DNA TechnologyDocument27 pagesDNA TechnologyIM CTNo ratings yet
- NT02 2122Document34 pagesNT02 2122Aadrit VatsNo ratings yet
- C. Elegans Genetic PortaitDocument26 pagesC. Elegans Genetic PortaitbelovedaffectionNo ratings yet
- Dneasy Powersoil Kit Handbook: For The Isolation of Microbial Genomic Dna From All Soil TypesDocument24 pagesDneasy Powersoil Kit Handbook: For The Isolation of Microbial Genomic Dna From All Soil TypesMaria MontoyaNo ratings yet
- One Taq DNAPolDocument2 pagesOne Taq DNAPolMuni SwamyNo ratings yet
- Existation Universal Molecular: Diagnostic SystemDocument6 pagesExistation Universal Molecular: Diagnostic SystemSubhanullah JalalNo ratings yet
- Textbook Introduction To Experimental Biophysics Second Edition Biological Methods For Physical Scientists Jay L Nadeau Ebook All Chapter PDFDocument54 pagesTextbook Introduction To Experimental Biophysics Second Edition Biological Methods For Physical Scientists Jay L Nadeau Ebook All Chapter PDFneal.hernandez911100% (11)
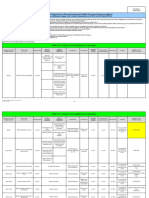
- Covid19 Diagnostic Products List - enDocument59 pagesCovid19 Diagnostic Products List - enVickyNo ratings yet
- GTI Manual Final 25juneDocument135 pagesGTI Manual Final 25juneoscarnicolasNo ratings yet