You might also like
- Resurge VSL ScriptDocument13 pagesResurge VSL ScriptsmithNo ratings yet
- MRSADocument44 pagesMRSAMarion PerniaNo ratings yet
- Microbiology CaseDocument3 pagesMicrobiology Caseclower112100% (2)
- Modul Hematoimun (Dr. Fakhri) - Immunity To Parasitic InfectionsDocument17 pagesModul Hematoimun (Dr. Fakhri) - Immunity To Parasitic InfectionsFajr Muzammil100% (1)
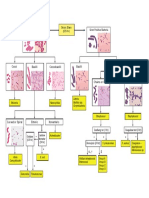
- Bacteria Classification FlowchartDocument1 pageBacteria Classification FlowchartLindsayNo ratings yet
- Forensic ToxicologyDocument165 pagesForensic Toxicologyapi-3763814100% (5)
- Sejarah Klasifikasi Antibiotik Dewi - 2017Document58 pagesSejarah Klasifikasi Antibiotik Dewi - 2017dr.syafril SpJPNo ratings yet
- WEEK 9 Sterilization & DisinfectionDocument38 pagesWEEK 9 Sterilization & DisinfectionotaibynaifNo ratings yet
- VibrioDocument32 pagesVibrioVishnuKumarNo ratings yet
- 1 Staphylococcus Lecture 1 Last YearDocument39 pages1 Staphylococcus Lecture 1 Last YearKeshant Samaroo100% (1)
- Praktikum Mikrobiologi Gram NegatifDocument44 pagesPraktikum Mikrobiologi Gram Negatifrids_No ratings yet
- Microbiology MUHS Questions (2005-2015)Document4 pagesMicrobiology MUHS Questions (2005-2015)Shahid KhanNo ratings yet
- Mycobacteria BPTDocument26 pagesMycobacteria BPTbpt2No ratings yet
- Giardia PPT M.SC Medical 4th SemDocument16 pagesGiardia PPT M.SC Medical 4th SemRahul ChaudharyNo ratings yet
- Level 3Document9 pagesLevel 3Zain HadiNo ratings yet
- SalmonellaDocument23 pagesSalmonellaahmedtwanaahmedNo ratings yet
- Virulence Factor of E. ColiDocument26 pagesVirulence Factor of E. ColiNazii Baig100% (1)
- ESBLDocument11 pagesESBLdianaNo ratings yet
- Bacte Day 2Document24 pagesBacte Day 2Jadey InfanteNo ratings yet
- Microbial Spoilage B Pharma 305 TDocument28 pagesMicrobial Spoilage B Pharma 305 TAbrar AnsariNo ratings yet
- MycetomaDocument26 pagesMycetomaTummalapalli Venkateswara RaoNo ratings yet
- Scrub Typhus: The Re-Emerging Threat - Thesis SynopsisDocument17 pagesScrub Typhus: The Re-Emerging Threat - Thesis SynopsisRajesh PadhiNo ratings yet
- Lab Diagnosis - ExclusiveDocument135 pagesLab Diagnosis - ExclusivesaaNo ratings yet
- Medical Microbiology For GraduatesDocument64 pagesMedical Microbiology For Graduatestummalapalli venkateswara rao100% (1)
- Applied Microbiology Fall 2015Document56 pagesApplied Microbiology Fall 2015Le HungNo ratings yet
- Medical Microbiology LEC 2 PDFDocument20 pagesMedical Microbiology LEC 2 PDFيوسف عسكرNo ratings yet
- Prepared by Suzette B. Doctolero: Acinetobacter, Stenotrophomonas, andDocument16 pagesPrepared by Suzette B. Doctolero: Acinetobacter, Stenotrophomonas, andPojangNo ratings yet
- Genera:: Treponema & BorreiliaDocument25 pagesGenera:: Treponema & BorreiliaKhalifa Sifaw Ghenghesh100% (1)
- Bacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityDocument20 pagesBacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityYogiabrorNo ratings yet
- Resistensi AntibiotikaDocument55 pagesResistensi AntibiotikaDavid Cahyo WibisonoNo ratings yet
- Discuss The Various Theories On The Gram Stain.: Gram-Negative Bacteria Gram-Positive BacteriaDocument5 pagesDiscuss The Various Theories On The Gram Stain.: Gram-Negative Bacteria Gram-Positive BacteriaFiddo Waggay100% (3)
- Tumor Marker GUPERDocument15 pagesTumor Marker GUPERyessiNo ratings yet
- 3 MicrobialNutritionGrowthDocument100 pages3 MicrobialNutritionGrowthHanzel GarcitosNo ratings yet
- 2-Microscopic IdentificationDocument24 pages2-Microscopic IdentificationMunir AhmedNo ratings yet
- Mycobacterium Leprae: DR Retno Budiarti Microbiology DepartmentDocument25 pagesMycobacterium Leprae: DR Retno Budiarti Microbiology DepartmentPrincess QumanNo ratings yet
- Medical MycologyDocument1 pageMedical MycologyHairul AnuarNo ratings yet
- Microbiology MUHS Questions (2005-2015) : VirologyDocument7 pagesMicrobiology MUHS Questions (2005-2015) : VirologyShahid KhanNo ratings yet
- Microbiology PosterDocument1 pageMicrobiology PosterAgnieszkaNo ratings yet
- Lecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)Document45 pagesLecture 27-Basic Virology-Dr. Ludhang Pradipta Rizki, M.biotech, SP - MK (2018)NOVI UMAMI UMAMINo ratings yet
- Streptococcus Pyogenes (GAS) : Common Characteristics Virulence Factors, Diseases and Key TestsDocument5 pagesStreptococcus Pyogenes (GAS) : Common Characteristics Virulence Factors, Diseases and Key TestsAmador GielasNo ratings yet
- Pulmonary Tuberculosis: June 2008Document2 pagesPulmonary Tuberculosis: June 2008kamalab04No ratings yet
- Family EnterobacteriaceaeDocument8 pagesFamily EnterobacteriaceaeWynlor AbarcaNo ratings yet
- Secondary MetabolliteDocument20 pagesSecondary MetabolliteChindieyciiEy Lebaiey CwekZrdoghNo ratings yet
- Historical Development of Medical MicrobiologyDocument84 pagesHistorical Development of Medical MicrobiologyH.K. DL67% (3)
- Subcutaneous MycosesDocument16 pagesSubcutaneous MycosesNazaqat FarooqNo ratings yet
- Mycobacterium Tuberculosis and Tuberculosis - TodarDocument18 pagesMycobacterium Tuberculosis and Tuberculosis - TodarTanti Dewi WulantikaNo ratings yet
- Tes Lab Penyakit Infeksi Dan Tropis (April 2011)Document143 pagesTes Lab Penyakit Infeksi Dan Tropis (April 2011)Fajrul AnsarNo ratings yet
- ENTEROBACTERIACEAEDocument23 pagesENTEROBACTERIACEAEapi-19916399No ratings yet
- LJ MediaDocument3 pagesLJ MediaJerry ThompsonNo ratings yet
- Nosocomial Infection.2Document19 pagesNosocomial Infection.2Antonius SbbrNo ratings yet
- Urine Sediment Particles PDFDocument119 pagesUrine Sediment Particles PDFambadepravinNo ratings yet
- Pseudomonas Aeruginosa: Name: Beltran, Regine B. BSN 101Document6 pagesPseudomonas Aeruginosa: Name: Beltran, Regine B. BSN 101Kyedae ShymkoNo ratings yet
- Clostrdia: G Positive Spore Forming Anaerobic Toxin Producing RodsDocument36 pagesClostrdia: G Positive Spore Forming Anaerobic Toxin Producing Rodsjamal nasirNo ratings yet
- Introduction To BacteriologyDocument45 pagesIntroduction To BacteriologyREIGN MARIE S. MARIANONo ratings yet
- Albert Staining (Pewarnaan Granula)Document4 pagesAlbert Staining (Pewarnaan Granula)SALSABILA AMANIANo ratings yet
- TCBS Agar PDFDocument2 pagesTCBS Agar PDFJhudit Camacho100% (1)
- Multiple Drug ResistanceDocument14 pagesMultiple Drug ResistanceHarsh ChopraNo ratings yet
- Corynebacterium DiphtheriaeDocument14 pagesCorynebacterium DiphtheriaedrparachuruNo ratings yet
- 2016 Antifungal Agent Full PDFDocument16 pages2016 Antifungal Agent Full PDFyeni novi yantiNo ratings yet
- Gene Expression: Protein Synthesis and Control RNA Synthesis and Control Chromatin Structure and FunctionFrom EverandGene Expression: Protein Synthesis and Control RNA Synthesis and Control Chromatin Structure and FunctionBrian F. C. ClarkNo ratings yet
- Hydrex 6316-EnDocument1 pageHydrex 6316-EnSayed SalahNo ratings yet
- Tugas Individu Non Blok English Medic "?": OlehDocument4 pagesTugas Individu Non Blok English Medic "?": OlehKhamid LujanNo ratings yet
- Hugh Jackman's Workout - Strong, Lean & PowerfulDocument14 pagesHugh Jackman's Workout - Strong, Lean & PowerfulMouh100% (1)
- 11-Iv Admixture 0Document20 pages11-Iv Admixture 0udinNo ratings yet
- The Effects of Drinking Alcoholic Drinks Among College StudentsDocument7 pagesThe Effects of Drinking Alcoholic Drinks Among College StudentsJohn Remar SilmaroNo ratings yet
- Taping and Wrapping: Sports MedicineDocument34 pagesTaping and Wrapping: Sports Medicinewong yoke hinNo ratings yet
- Chemical Approval ProcessDocument5 pagesChemical Approval ProcessGiovanniNo ratings yet
- Aish Tipsheet Employment IncomeDocument2 pagesAish Tipsheet Employment IncomePhilip CherianNo ratings yet
- Community Wishbook 2019-2020Document40 pagesCommunity Wishbook 2019-2020Darlyn ReddyNo ratings yet
- 2017 Journals (Including Open Access)Document227 pages2017 Journals (Including Open Access)mazhaicNo ratings yet
- Disadvantages of Life InsuranceDocument1 pageDisadvantages of Life InsuranceAjay GuptaNo ratings yet
- Internalized Homophobia and Health Issues Affecting Lesbians and Gay MenDocument11 pagesInternalized Homophobia and Health Issues Affecting Lesbians and Gay Menushha2No ratings yet
- Personality Disorders - A Brief OverviewDocument2 pagesPersonality Disorders - A Brief OverviewMaria- AndreeaNo ratings yet
- Thesis Rajiv Gandhi UniversityDocument8 pagesThesis Rajiv Gandhi Universityafcmqldsw100% (2)
- GRCHRT Girls 24LW 9210Document1 pageGRCHRT Girls 24LW 9210Stephen GregorNo ratings yet
- Pco Accreditation FormDocument3 pagesPco Accreditation FormJan GarciaNo ratings yet
- Montana Marijuana InitiativesDocument38 pagesMontana Marijuana InitiativesMarijuana Moment100% (1)
- Contact No: 016-236 2504 Personal ParticularsDocument6 pagesContact No: 016-236 2504 Personal ParticularsMALINA NEELVILINo ratings yet
- Dr. Farsalinos' Study On Diacetyl and Acetyl Propionyl in E-LiquidDocument28 pagesDr. Farsalinos' Study On Diacetyl and Acetyl Propionyl in E-LiquidRuss WishtartNo ratings yet
- The Physical Fitness Training Plan With 6 Handouts AttachedDocument20 pagesThe Physical Fitness Training Plan With 6 Handouts AttachedMuz ZakiNo ratings yet
- Yoga For Blissful HealthDocument3 pagesYoga For Blissful HealthUmmesalama ManasawalaNo ratings yet
- (Artigo) (Anatomia) Gastroduodenal Artery - Single Key For Many Locks Desai (2019)Document11 pages(Artigo) (Anatomia) Gastroduodenal Artery - Single Key For Many Locks Desai (2019)Beatriz BelottiNo ratings yet
- CAE Use of English Part 5 - Key Word TransformationDocument5 pagesCAE Use of English Part 5 - Key Word TransformationAndreaGarciaRuzNo ratings yet
- Surgical Site MarkingDocument12 pagesSurgical Site Markingh1m4w4nNo ratings yet
- Hubungan Letak Lesi Dengan Derajat Spastisitas Pada Pasien Stroke Iskemik Di Rsud Ulin BanjarmasinDocument8 pagesHubungan Letak Lesi Dengan Derajat Spastisitas Pada Pasien Stroke Iskemik Di Rsud Ulin BanjarmasinniekoNo ratings yet
- Deuxieme MagasinDocument5 pagesDeuxieme MagasinYacouba DembeleNo ratings yet
- Wk3 Slideshow Acute Responses To ExerciseDocument19 pagesWk3 Slideshow Acute Responses To Exercisejademcmahon0210100% (2)
- Neela DoggDocument28 pagesNeela Doggakash kumarNo ratings yet