You might also like
- SGL Case 31 - Study GuideDocument20 pagesSGL Case 31 - Study GuidebangityNo ratings yet
- Kefir RecipesDocument109 pagesKefir RecipesCaja Huz100% (5)
- Option StrategiesDocument13 pagesOption StrategiesArunangshu BhattacharjeeNo ratings yet
- The Vital Problems of Pistol ShootingDocument15 pagesThe Vital Problems of Pistol Shootingapi-3695814100% (4)
- Management of Patients With Oral and Esophageal Disorders PDFDocument85 pagesManagement of Patients With Oral and Esophageal Disorders PDFNixi Mbuthia100% (3)
- Hongkong v. Olalia, Jr. (CASE DIGEST)Document3 pagesHongkong v. Olalia, Jr. (CASE DIGEST)Samantha NicoleNo ratings yet
- Case Report MTH HydroceleDocument9 pagesCase Report MTH Hydrocelesamuel_hildaNo ratings yet
- Salivary Gland DisordersDocument50 pagesSalivary Gland DisordersghazyNo ratings yet
- Salivary GlandDocument64 pagesSalivary GlandDanielicah Cruz100% (1)
- Submandibular Salivary Sialolith: A Case Report With Review of LiteratureDocument4 pagesSubmandibular Salivary Sialolith: A Case Report With Review of LiteraturejoaompradoNo ratings yet
- Case Report: Sialolithiasis of The Wharton 'S Duct - Report of 3 CasesDocument4 pagesCase Report: Sialolithiasis of The Wharton 'S Duct - Report of 3 CasesSukhvinder Singh RanaNo ratings yet
- SialolithiasisDocument4 pagesSialolithiasisMiftah WiryaniNo ratings yet
- Ipm 3Document4 pagesIpm 3rochmandrg dokter gigiNo ratings yet
- SialolithDocument19 pagesSialolithShyam BhatNo ratings yet
- (2020-2021) Salivary Gland DiseasesDocument5 pages(2020-2021) Salivary Gland DiseasesQueen LiveNo ratings yet
- Sialolithiasis - A Report of Two Cases and ReviewDocument4 pagesSialolithiasis - A Report of Two Cases and Reviewmaharani spNo ratings yet
- ContempClinDent4178-3521414 - 094654 (CASE)Document3 pagesContempClinDent4178-3521414 - 094654 (CASE)Fahmi FirmansyahNo ratings yet
- Salivary Gland Dysfunction: Etiology, Epidemiology, Clinical Manifestations, Diagnosis, and TreatmentDocument20 pagesSalivary Gland Dysfunction: Etiology, Epidemiology, Clinical Manifestations, Diagnosis, and TreatmentMonaNo ratings yet
- Bing Skenario 3Document12 pagesBing Skenario 3Anonymous bj9EmmtNo ratings yet
- 44 Danfulani EtalDocument3 pages44 Danfulani EtaleditorijmrhsNo ratings yet
- Etm 11 1 335 PDFDocument3 pagesEtm 11 1 335 PDFjoaompradoNo ratings yet
- Salivary Duct Stenosis Diagnosis and TreatmentDocument10 pagesSalivary Duct Stenosis Diagnosis and TreatmentYeni PuspitasariNo ratings yet
- Sialolithiasis: Vi Ugboko Fmcds FwacsDocument47 pagesSialolithiasis: Vi Ugboko Fmcds FwacsAkeem Alawode50% (2)
- Clinical Case: Removal of A Giant Sialolith Using The Transoral ApproachDocument7 pagesClinical Case: Removal of A Giant Sialolith Using The Transoral ApproachmatharoorupinderNo ratings yet
- Lec 19 DISEASES OF THE SALIVARY GLANDDocument17 pagesLec 19 DISEASES OF THE SALIVARY GLANDpxb8dhqgs9No ratings yet
- A Huge Oral Ranula: Moosa BahnassyDocument2 pagesA Huge Oral Ranula: Moosa BahnassyAriska EndariantariNo ratings yet
- Intussusception: Read By: Krisna (KNA)Document26 pagesIntussusception: Read By: Krisna (KNA)krisnaNo ratings yet
- Mucocele Ranula Sialolithiasis SialoadenitisDocument4 pagesMucocele Ranula Sialolithiasis SialoadenitisNegin HekmatjooNo ratings yet
- 31 Uro Hydrocele 111211112520 Phpapp02Document6 pages31 Uro Hydrocele 111211112520 Phpapp02ppc_20No ratings yet
- Jenis Jenis LukaDocument4 pagesJenis Jenis LukaMuchtar RezaNo ratings yet
- Multiple Bilateral Submandibular Gland Sialolithiasis: Case ReportDocument4 pagesMultiple Bilateral Submandibular Gland Sialolithiasis: Case Reportarief satrioNo ratings yet
- Haemorrhoidsb 06Document3 pagesHaemorrhoidsb 06Ngu Ing SoonNo ratings yet
- Small Nowel Emergency SurgeryDocument8 pagesSmall Nowel Emergency SurgerySurya Nirmala DewiNo ratings yet
- Jurnal BM DittaDocument4 pagesJurnal BM DittaRyans FkdokgiNo ratings yet
- MNJJDocument12 pagesMNJJFadhli AzhimiNo ratings yet
- Oral Tori in Chronic Hemodialysis PatientsDocument7 pagesOral Tori in Chronic Hemodialysis PatientsAbdul Rahman AlmishhdanyNo ratings yet
- Nasopalatine Duct CystDocument4 pagesNasopalatine Duct CystVikneswaran Vîçký100% (1)
- Maat 12 I 3 P 271 DDDDDocument5 pagesMaat 12 I 3 P 271 DDDDKacamata BagusNo ratings yet
- Disease of RectumDocument22 pagesDisease of RectumTalal AbbasiNo ratings yet
- Plunging Ranula: A Case ReportDocument5 pagesPlunging Ranula: A Case ReportNadillaNo ratings yet
- Mucocele On The Lower Lip Treated by Scalpel Excision Method-A CaseDocument5 pagesMucocele On The Lower Lip Treated by Scalpel Excision Method-A CaseGea Akalili SabrinaNo ratings yet
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDocument3 pagesFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiNo ratings yet
- Life Sci. JDocument11 pagesLife Sci. JDanis Diba Sabatillah YaminNo ratings yet
- SialodenosisDocument76 pagesSialodenosisJessica GreenNo ratings yet
- Kelenjar BartoliniDocument15 pagesKelenjar BartolinionlyfellaNo ratings yet
- Basics of Intestinal Surgery: Anatomy, Pathophysiology, Instrumentation & SuturingDocument8 pagesBasics of Intestinal Surgery: Anatomy, Pathophysiology, Instrumentation & SuturingakreditasirsurNo ratings yet
- Jurnalku OsccDocument4 pagesJurnalku OsccAndiOctafiantoNo ratings yet
- 984 Pediatric Hernias and Hydrocele Pediatric SurgeryDocument27 pages984 Pediatric Hernias and Hydrocele Pediatric SurgeryVijay KumarNo ratings yet
- Management of Extra Oral Sinus Tract Associated With Large Periapical Lesion - A Case ReportDocument1 pageManagement of Extra Oral Sinus Tract Associated With Large Periapical Lesion - A Case ReportNgân PhạmNo ratings yet
- Scientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportDocument6 pagesScientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportSasa AprilaNo ratings yet
- Percutaneous Nephrolithotomy AbstractDocument10 pagesPercutaneous Nephrolithotomy AbstractTrifan_DumitruNo ratings yet
- Case ReportDocument3 pagesCase ReportZahra HayunaNo ratings yet
- Kelenjar BartoliniDocument15 pagesKelenjar BartolinionlyfellaNo ratings yet
- Augmentation Bladder KomplikasiDocument9 pagesAugmentation Bladder KomplikasiOlivia BawaedaNo ratings yet
- Indications and Complications of Intestinal Stomas - A Tertiary Care Hospital ExperienceDocument4 pagesIndications and Complications of Intestinal Stomas - A Tertiary Care Hospital ExperienceOliviaNo ratings yet
- Acute Submandibular Sialadenitis-A Case ReportDocument4 pagesAcute Submandibular Sialadenitis-A Case ReportsurgaNo ratings yet
- Recent Advancements in Management of Alveolar Osteitis (Dry Socket)Document5 pagesRecent Advancements in Management of Alveolar Osteitis (Dry Socket)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Magnetic Marker Monitoring Allows To Characterize Effects of Exogenous Factors On Esophageal Transit of Solid Drug FormsDocument3 pagesMagnetic Marker Monitoring Allows To Characterize Effects of Exogenous Factors On Esophageal Transit of Solid Drug FormsSaravanan MathiNo ratings yet
- Xerostomia: Faktor Etiologi. Etiologi Dan PenanggulanganDocument8 pagesXerostomia: Faktor Etiologi. Etiologi Dan PenanggulanganJonathan JojoNo ratings yet
- Gigi Dan MulutDocument6 pagesGigi Dan MulutnurfitriaNo ratings yet
- Light Blue Creative Modern Medical Clinic PresentationDocument40 pagesLight Blue Creative Modern Medical Clinic Presentationمحمد عقيل عبد الامير ستارNo ratings yet
- Vol06 b2 37-40strDocument4 pagesVol06 b2 37-40strDentist HereNo ratings yet
- Clinical Management of Bowel Endometriosis: From Diagnosis to TreatmentFrom EverandClinical Management of Bowel Endometriosis: From Diagnosis to TreatmentSimone FerreroNo ratings yet
- EXPERT-JSA Structural, Piping & Welding WorksDocument9 pagesEXPERT-JSA Structural, Piping & Welding Worksarun vijayNo ratings yet
- Anatomy Embryology 1&2Document39 pagesAnatomy Embryology 1&2Nadeen ShahwanNo ratings yet
- Konsep New PedagogyDocument14 pagesKonsep New PedagogyNUR IZZATI BINTI MOHAMAD SABRI KPM-GuruNo ratings yet
- Industrial Cutters: Elaborate Concept Enhancing Your ProductivityDocument11 pagesIndustrial Cutters: Elaborate Concept Enhancing Your ProductivityMoreno markovicNo ratings yet
- Jts Templates For JosephDocument41 pagesJts Templates For JosephCharlie M LozaritaNo ratings yet
- Homework Not Done Note ParentsDocument8 pagesHomework Not Done Note Parentsafnaoabfuddcdf100% (1)
- English Mania by Jay Walker: Watching and ListeningDocument2 pagesEnglish Mania by Jay Walker: Watching and ListeningRandom XYZNo ratings yet
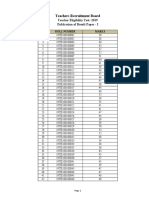
- ResultPaperI PDFDocument3,868 pagesResultPaperI PDFRavikumarNo ratings yet
- Total Quality Management Multiple Choice Questions and Answers. Page 7Document3 pagesTotal Quality Management Multiple Choice Questions and Answers. Page 7Prakash prajapatiNo ratings yet
- (H) - Sem6 - BCH 6.4 (D) - Industrial Relations and Labour Laws - W2 - CG - UNIT 5 - 0Document54 pages(H) - Sem6 - BCH 6.4 (D) - Industrial Relations and Labour Laws - W2 - CG - UNIT 5 - 0sanchiNo ratings yet
- WNC1800ZFR182x Pro Series Wireless PDFDocument70 pagesWNC1800ZFR182x Pro Series Wireless PDFrohit sharmaNo ratings yet
- 24 Global Currency Fund Mid-May 2020 Term SheetDocument1 page24 Global Currency Fund Mid-May 2020 Term SheeterdNo ratings yet
- J Matpr 2021 06 081Document8 pagesJ Matpr 2021 06 081SREEJITH S NAIR100% (1)
- Crimethinc - Fighting For OurlivesDocument13 pagesCrimethinc - Fighting For OurlivesHCaruthersIsDeadNo ratings yet
- Bio - Data FormDocument9 pagesBio - Data FormPrathmesh GujaratiNo ratings yet
- Linuxengines Blogspot inDocument9 pagesLinuxengines Blogspot inShitesh SachanNo ratings yet
- Mystici Corporis Christi (1943)Document38 pagesMystici Corporis Christi (1943)Jennifer R. RustNo ratings yet
- DCMMMNHS - Work Immersion Proper and Post ImmersionDocument3 pagesDCMMMNHS - Work Immersion Proper and Post ImmersionTresita B. RiosNo ratings yet
- Barachini 2009Document14 pagesBarachini 2009testchoithoi1No ratings yet
- Main MenuDocument3 pagesMain MenueatlocalmenusNo ratings yet
- Chapter 15 - Air ConditioningDocument121 pagesChapter 15 - Air ConditioningWawNo ratings yet
- Unit 34 Digital Marketing - LO2Document14 pagesUnit 34 Digital Marketing - LO2Nabeel hassanNo ratings yet
- Nef Upper Filetest 02 Answerkey PDFDocument6 pagesNef Upper Filetest 02 Answerkey PDFCoralza SacNo ratings yet
- 1 DSKP KSSR Bi Year 1 SK - 2018Document3 pages1 DSKP KSSR Bi Year 1 SK - 2018aziawati ahmadNo ratings yet
- Dolphin Station - Pre App Letter of IntentDocument3 pagesDolphin Station - Pre App Letter of Intentthe next miamiNo ratings yet