You might also like
- NUR 151 P1 EXAM REVIEWDocument13 pagesNUR 151 P1 EXAM REVIEWJilkiah Mae Alfoja Campomanes100% (2)
- ITOM Group Assignment Issues at SCHDocument12 pagesITOM Group Assignment Issues at SCHzeeraNo ratings yet
- Clinical Study of Urolithiasis Management in Rural HospitalDocument11 pagesClinical Study of Urolithiasis Management in Rural HospitalLusi RustinaNo ratings yet
- Delivery of Huge Bladder Stone in A Thirty-Five-Year-Old ManDocument3 pagesDelivery of Huge Bladder Stone in A Thirty-Five-Year-Old ManJetsinNo ratings yet
- Jurnal UrolithiasisDocument6 pagesJurnal UrolithiasisAliimah KhairiyahNo ratings yet
- Should Ureteroscopy Be Considered As The First Choice For Proximal Ureter Stones of Children?Document6 pagesShould Ureteroscopy Be Considered As The First Choice For Proximal Ureter Stones of Children?TheQueensafa90No ratings yet
- 44 Danfulani EtalDocument3 pages44 Danfulani EtaleditorijmrhsNo ratings yet
- E0142528 LibreDocument4 pagesE0142528 LibreArsy Mira PertiwiNo ratings yet
- Modern Management of Pyogenic Hepatic Abscess: A Case Series and Review of The LiteratureDocument8 pagesModern Management of Pyogenic Hepatic Abscess: A Case Series and Review of The LiteratureAstari Pratiwi NuhrintamaNo ratings yet
- Prevalence of Biliary Ascariasis and ItsDocument2 pagesPrevalence of Biliary Ascariasis and ItsProf Dr S M Moinul IslamNo ratings yet
- Nephrolithiasis and Obstruction: Key PointsDocument6 pagesNephrolithiasis and Obstruction: Key PointsSyarifHusinNo ratings yet
- JVC 38 2 63Document6 pagesJVC 38 2 63dpcamposhNo ratings yet
- Jsap 12996Document6 pagesJsap 12996dpcamposhNo ratings yet
- Microscopic Investigations of Urine of Sickle Cell Anemic PatientsDocument6 pagesMicroscopic Investigations of Urine of Sickle Cell Anemic PatientsTJPRC PublicationsNo ratings yet
- Renal Calyceal MicrolithiasisDocument3 pagesRenal Calyceal MicrolithiasisVic L. AmecaNo ratings yet
- Research: The Profile of Patients With Obstructive Uropathy in Cameroon: Case of The Douala General HospitalDocument6 pagesResearch: The Profile of Patients With Obstructive Uropathy in Cameroon: Case of The Douala General HospitalSidan EmozieNo ratings yet
- 7399 14545 1 SM PDFDocument6 pages7399 14545 1 SM PDFTaffy GultomNo ratings yet
- Feijão e Cálculos renaisDocument11 pagesFeijão e Cálculos renaisEmily FerreiraNo ratings yet
- Prevalence of Variceal Bleeding in ALD PatientsDocument5 pagesPrevalence of Variceal Bleeding in ALD PatientsvarishNo ratings yet
- Urinary 1Document7 pagesUrinary 1Yuni AstutiNo ratings yet
- Chemical Analysis of Stones and Its Significance in UrolithiasisDocument8 pagesChemical Analysis of Stones and Its Significance in UrolithiasisNithya sudevNo ratings yet
- Tips and Tricks in Laparoscopic Ureterolithotomy For Large Ureteric Stones About 8 CasesDocument4 pagesTips and Tricks in Laparoscopic Ureterolithotomy For Large Ureteric Stones About 8 CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IJVM - Volume 12 - Issue 4 - Pages 293-303Document11 pagesIJVM - Volume 12 - Issue 4 - Pages 293-303Violet Pet ClinicNo ratings yet
- Epidemiologi KolestasisDocument6 pagesEpidemiologi KolestasisDominikus Raditya AtmakaNo ratings yet
- Pediatric Urolithiasis: Experience at A Tertiary Care Pediatric HospitalDocument12 pagesPediatric Urolithiasis: Experience at A Tertiary Care Pediatric HospitalkristinaNo ratings yet
- 8 - Original GhorbaniDocument6 pages8 - Original GhorbaniNaziheh AssarzadeganNo ratings yet
- Urolithiasis (Definisi)Document7 pagesUrolithiasis (Definisi)Putri AndiraNo ratings yet
- Measure BUN Creat urine leakageDocument4 pagesMeasure BUN Creat urine leakagerendi wibowoNo ratings yet
- Urethral Obstruction in Cats: Predisposing Factors, Clinical, Clinicopathological Characteristics and PrognosisDocument8 pagesUrethral Obstruction in Cats: Predisposing Factors, Clinical, Clinicopathological Characteristics and PrognosisGiulia DravelliNo ratings yet
- Recurrence StoneDocument7 pagesRecurrence Stonerafo18No ratings yet
- Prevalence of Anaemia in Decompensated Chronic Liver DiseaseDocument5 pagesPrevalence of Anaemia in Decompensated Chronic Liver DiseaseElang SudewaNo ratings yet
- S4mns 2010Document7 pagesS4mns 2010Ratna Puspa RahayuNo ratings yet
- ST Riner Sistem Ta Lar Nda ESWL Nin Etkinli I (#390504) - 419548Document6 pagesST Riner Sistem Ta Lar Nda ESWL Nin Etkinli I (#390504) - 419548Abeselom lemmaNo ratings yet
- Posterior Urethral Valves: Long-Term OutcomeDocument9 pagesPosterior Urethral Valves: Long-Term OutcomeRajarshi KumarNo ratings yet
- Revisiting The Predictive Factors For Intra-Op-erative Complications of Rigid UreterosDocument8 pagesRevisiting The Predictive Factors For Intra-Op-erative Complications of Rigid UreterosTatik HandayaniNo ratings yet
- The Bacterial Pattern in UTI at Kidney Stone (Jurnal)Document8 pagesThe Bacterial Pattern in UTI at Kidney Stone (Jurnal)venue_newNo ratings yet
- Case Report: Author DetailsDocument3 pagesCase Report: Author DetailsInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- A 12-Year Retrospective Study of Invasive Amoebiasis in Western Sydney: Evidence of Local AcquisitionDocument8 pagesA 12-Year Retrospective Study of Invasive Amoebiasis in Western Sydney: Evidence of Local AcquisitionAdistyDWNo ratings yet
- Types Sites and Causes of Mechanical Intestinal ObDocument5 pagesTypes Sites and Causes of Mechanical Intestinal ObPutra FebdianNo ratings yet
- Role of Transabdominal Ultrasound in Evaluating Patients With Acute Urinary Retention (Aur) Due To Benign Prostatic Hyperplasia (BPH)Document3 pagesRole of Transabdominal Ultrasound in Evaluating Patients With Acute Urinary Retention (Aur) Due To Benign Prostatic Hyperplasia (BPH)Yuni AngrianiNo ratings yet
- Biliary Atresia: Experience With 30 Consecutive Cases in A Single InstituteDocument8 pagesBiliary Atresia: Experience With 30 Consecutive Cases in A Single Institutemisbahhari_mdNo ratings yet
- Barret 2015.Document6 pagesBarret 2015.Elizabeth VegaNo ratings yet
- Splenectomy Is A Risk Factor For Developing Hyperuricemia and Nephrolithiasis in PDFDocument3 pagesSplenectomy Is A Risk Factor For Developing Hyperuricemia and Nephrolithiasis in PDFDayanne TeixeiraNo ratings yet
- Management of Liver Abscess in Children: Our Experience: 10.5005/jp-Journals-10018-1206Document4 pagesManagement of Liver Abscess in Children: Our Experience: 10.5005/jp-Journals-10018-1206Ivan VeriswanNo ratings yet
- Original Article Urethral Cultures in Patients With Spinal Cord InjuryDocument5 pagesOriginal Article Urethral Cultures in Patients With Spinal Cord InjuryAkhmad Rizky SubkiNo ratings yet
- Jurnal Sitologi UrineDocument10 pagesJurnal Sitologi UrineAjip JenNo ratings yet
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 pagesAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaNo ratings yet
- Jurnal Bedah - Elsy MulyaDocument14 pagesJurnal Bedah - Elsy MulyaariesfadhliNo ratings yet
- Risk factors for carcinogenesis in choledochal cyst patientsF/491Gender/AgeTodanitypeTable 1. Clinical characteristics of 15 patients with malignant tumors arising from choledochal cystsDocument8 pagesRisk factors for carcinogenesis in choledochal cyst patientsF/491Gender/AgeTodanitypeTable 1. Clinical characteristics of 15 patients with malignant tumors arising from choledochal cystsDaphne Ongbit JaritoNo ratings yet
- Open Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132 PDFDocument3 pagesOpen Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132 PDFSarah ValdezNo ratings yet
- Obstructive NephropathyDocument4 pagesObstructive NephropathyKevean Kimi LimNo ratings yet
- The Prevalence and Clinical Characteristics of Adult Polycystic Kidney Disease in Ilorin, NigeriaDocument5 pagesThe Prevalence and Clinical Characteristics of Adult Polycystic Kidney Disease in Ilorin, NigeriaMuhammad A MakusidiNo ratings yet
- Urinary_Tract_Infection_in_Hemodialysis-Dependent_Document9 pagesUrinary_Tract_Infection_in_Hemodialysis-Dependent_rada taniaNo ratings yet
- Renal Tubular Acidosis PDFDocument7 pagesRenal Tubular Acidosis PDFishtiaq ahmadNo ratings yet
- Bệnh Lý KNBTNQ (Tài Liệu Báo Cáo)Document8 pagesBệnh Lý KNBTNQ (Tài Liệu Báo Cáo)Nguyễn Văn KhoaNo ratings yet
- A Clinicopathological Study of Cholelithiasis in An Eastern Indian PopulationDocument7 pagesA Clinicopathological Study of Cholelithiasis in An Eastern Indian PopulationMeyva SasmitaNo ratings yet
- Ecgds 09 00916Document4 pagesEcgds 09 00916Houda El MoufidNo ratings yet
- Pattern of Acute Renal Failure at A Referral HospitalDocument7 pagesPattern of Acute Renal Failure at A Referral HospitalminhajulqowimNo ratings yet
- Cel Tumorales Mostoles 2008-CytopathologyDocument4 pagesCel Tumorales Mostoles 2008-CytopathologygemaNo ratings yet
- Study of Prevalence of Urinary Tract Infections in Patients of Ujjain Madhya Pradesh India - November - 2020 - 4619534901 - 1833083Document3 pagesStudy of Prevalence of Urinary Tract Infections in Patients of Ujjain Madhya Pradesh India - November - 2020 - 4619534901 - 1833083Sohrab RohaneNo ratings yet
- Manish Synopsis1 EditDocument13 pagesManish Synopsis1 EditManish kumar gurjarNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet
- Abnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsDocument3 pagesAbnormal Uterine Bleeding: Frequently Asked Questions FAQ095 Gynecologic ProblemsErwinNo ratings yet
- Association Between Smoking Behavior and LDLDocument1 pageAssociation Between Smoking Behavior and LDLSri Nowo MinartiNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaSri Nowo MinartiNo ratings yet
- Weight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Document1 pageWeight-For-Age GIRLS: 2 To 5 Years (Z-Scores)Gibson HorasNo ratings yet
- Nephrotic Syndrome in Adults 2009Document6 pagesNephrotic Syndrome in Adults 2009Mutiara RizkyNo ratings yet
- Management of Protozoal Diarrhoea in HIV DiseaseDocument6 pagesManagement of Protozoal Diarrhoea in HIV DiseaseSri Nowo MinartiNo ratings yet
- Management of Protozoal Diarrhoea in HIV DiseaseDocument6 pagesManagement of Protozoal Diarrhoea in HIV DiseaseSri Nowo MinartiNo ratings yet
- Nkcells Further ReadDocument1 pageNkcells Further ReadSri Nowo MinartiNo ratings yet
- Cover Skripsi Bahasa InggrisDocument1 pageCover Skripsi Bahasa InggrisSri Nowo MinartiNo ratings yet
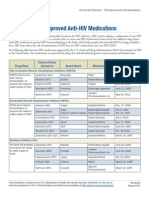
- ApprovedMedstoTreatHIV FS enDocument2 pagesApprovedMedstoTreatHIV FS enSri Nowo MinartiNo ratings yet
- Eur Heart J 2003 Fröhlich 1365 72Document8 pagesEur Heart J 2003 Fröhlich 1365 72Sri Nowo MinartiNo ratings yet
- 0709Document4 pages0709Sri Nowo MinartiNo ratings yet
- Uroanalisis AnormalDocument13 pagesUroanalisis AnormalMyke EstradaNo ratings yet
- Alcohol 10 QuestionnaireDocument1 pageAlcohol 10 Questionnaireyash_magooNo ratings yet
- 55 259Document6 pages55 259Sri Nowo MinartiNo ratings yet
- Frequency of Renal Stone Disease in Patients With Urinary Tract InfectionDocument3 pagesFrequency of Renal Stone Disease in Patients With Urinary Tract InfectionSri Nowo MinartiNo ratings yet
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDocument1 pageCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiNo ratings yet
- Afroz - Lipid ProfileDocument6 pagesAfroz - Lipid ProfileSri Nowo MinartiNo ratings yet
- Uroanalisis AnormalDocument13 pagesUroanalisis AnormalMyke EstradaNo ratings yet
- Dysuria in AdultsDocument8 pagesDysuria in AdultsSi vis pacem...No ratings yet
- VancouverDocument11 pagesVancouverAndi Firman MubarakNo ratings yet
- Corrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.EDocument1 pageCorrections: Theodore J. Cicero, Ph.D. Matthew S. Ellis, M.P.ESri Nowo MinartiNo ratings yet
- Difco BBL Mueller Hinton Agar BrothDocument5 pagesDifco BBL Mueller Hinton Agar BrothSri Nowo MinartiNo ratings yet
- ResourceDocument5 pagesResourceSri Nowo MinartiNo ratings yet
- Am J Clin Nutr 2008 Kupka 1802 8Document7 pagesAm J Clin Nutr 2008 Kupka 1802 8Sri Nowo MinartiNo ratings yet
- Niacin MOADocument3 pagesNiacin MOASri Nowo Minarti100% (1)
- The Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematurityDocument6 pagesThe Effect of Human Recombinant Erythropoietin On Prevention of Anemia of PrematuritySri Nowo MinartiNo ratings yet
- EpoDocument15 pagesEpoSri Nowo MinartiNo ratings yet
- Etiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumDocument10 pagesEtiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumSri Nowo MinartiNo ratings yet
- Dengue Discharge PlanDocument6 pagesDengue Discharge PlanChayliu Bugo75% (4)
- Cotard Syndrome - A Review of a Rare but Severe Psychiatric ConditionDocument6 pagesCotard Syndrome - A Review of a Rare but Severe Psychiatric ConditionbraispmNo ratings yet
- Estimated Costs Related To The Birth of A Drug And/Or Alcohol Exposed BabyDocument15 pagesEstimated Costs Related To The Birth of A Drug And/Or Alcohol Exposed BabylosangelesNo ratings yet
- Medicare Initial Preventive Physical Examination Encounter Form ("Welcome To Medicare Physical")Document2 pagesMedicare Initial Preventive Physical Examination Encounter Form ("Welcome To Medicare Physical")B PNo ratings yet
- IM ITE D: Reading Sub-TestDocument20 pagesIM ITE D: Reading Sub-TestAlwin BrightNo ratings yet
- Principles of Energy MedicineDocument92 pagesPrinciples of Energy MedicineRenato Dalmacio100% (4)
- History TakingDocument55 pagesHistory TakingDeepika MahajanNo ratings yet
- J Oral Pathology Medicine - 2007 - Arduino - Herpes Simplex Virus Type 1 Infection Overview On RelevantDocument15 pagesJ Oral Pathology Medicine - 2007 - Arduino - Herpes Simplex Virus Type 1 Infection Overview On RelevantTestNo ratings yet
- Stilnox 10 MGDocument4 pagesStilnox 10 MGperkinstop2000No ratings yet
- Social Medicine Author Silvia Capíková, Michaela Kosticová, Ivan SolovicDocument184 pagesSocial Medicine Author Silvia Capíková, Michaela Kosticová, Ivan SolovicCarlos RodriguezNo ratings yet
- Cephalandra Indica: A Miracle of Nature: Dr. AT Senthil Kumar, Dr. N Prasath Rajan and Dr. S SathyaDocument3 pagesCephalandra Indica: A Miracle of Nature: Dr. AT Senthil Kumar, Dr. N Prasath Rajan and Dr. S SathyaPriya JainNo ratings yet
- Chapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument7 pagesChapter 38: Cardiovascular Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- The Allergenicity of Genetically Modi Fied Foods From Genetically Engineered CropsDocument12 pagesThe Allergenicity of Genetically Modi Fied Foods From Genetically Engineered Cropsben mayNo ratings yet
- PBL OsteomyelitisDocument27 pagesPBL OsteomyelitisNabilah SufianNo ratings yet
- Delivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialDocument5 pagesDelivery of Evidence-Based Treatment For Multiple Anxiety Disorders in Primary Care: A Randomized Controlled TrialRaja DarmawanNo ratings yet
- Expert in BGM & PoCT TechnologiesDocument16 pagesExpert in BGM & PoCT TechnologiesMalik AlnabhaniNo ratings yet
- All-On-4, For PatientsDocument28 pagesAll-On-4, For PatientsmmsbabakNo ratings yet
- زياد ٤Document43 pagesزياد ٤Ibrahim RamizNo ratings yet
- Polycythemia in NeonatesDocument12 pagesPolycythemia in NeonatesjethrochristopherNo ratings yet
- HX Taking of PeadiatricsDocument5 pagesHX Taking of PeadiatricsCahaya Al-Hazeenillah100% (1)
- Nrs 2002 Form PDF - Google SearchDocument1 pageNrs 2002 Form PDF - Google SearchsandeepNo ratings yet
- Archaeus 4Document107 pagesArchaeus 4terrythecensorNo ratings yet
- 3 - Evaluation and Management of Rheumatoid ArthritisDocument56 pages3 - Evaluation and Management of Rheumatoid ArthritisDwi Astika SariNo ratings yet
- Secrets of The SiddhasDocument1 pageSecrets of The SiddhasChiranth ChandNo ratings yet
- EAUN15 Guideline Intravesical InstillationDocument90 pagesEAUN15 Guideline Intravesical InstillationRafael RojasNo ratings yet
- Covid 19 Telehealth Program RecipientsDocument21 pagesCovid 19 Telehealth Program RecipientsEd Praetorian100% (1)
- Paul Farmer, Pioneer of Global Health, Dies at 62Document3 pagesPaul Farmer, Pioneer of Global Health, Dies at 62ALFINo ratings yet
- What Explains The Directionality of Flow in Health Care? Patients, Health Workers and Managerial Practices?Document7 pagesWhat Explains The Directionality of Flow in Health Care? Patients, Health Workers and Managerial Practices?Dancan OnyangoNo ratings yet