You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Twitter Class Action Lawsuit Over Mass LayoffsDocument10 pagesTwitter Class Action Lawsuit Over Mass LayoffsTechCrunchNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
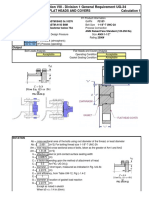
- ASME BPVC 2008a Section VIII - Division 1 General Requirement UG-34Document12 pagesASME BPVC 2008a Section VIII - Division 1 General Requirement UG-34akarczNo ratings yet
- Pala HidraulicaDocument163 pagesPala HidraulicaBerato Ramirez T100% (10)
- 4971233Document6 pages4971233jorgeroa111No ratings yet
- Condux Fiber Optic Cable PullerDocument32 pagesCondux Fiber Optic Cable PullerComstar SupplyNo ratings yet
- Gnpower Dinginin Ltd. Co. Operation and Maintenance Management Electrical Progress ReportDocument4 pagesGnpower Dinginin Ltd. Co. Operation and Maintenance Management Electrical Progress Reportpepenapao1217No ratings yet
- Salesforce CRM User Manual ST Francis ST MarksDocument28 pagesSalesforce CRM User Manual ST Francis ST Markslaxmisha1987No ratings yet
- 3.2 The - Lay - ReportsDocument237 pages3.2 The - Lay - Reportsdavidescu5costin33% (3)
- Recycled Chopping BoardDocument13 pagesRecycled Chopping BoardDejan RancicNo ratings yet
- Certificate ASSET DOC LOC 6801275Document1 pageCertificate ASSET DOC LOC 6801275Nyein ZawNo ratings yet
- Tugas 1 Menjaga Kesehatan TubuhhDocument9 pagesTugas 1 Menjaga Kesehatan TubuhhDiah Dwi NursyaidahNo ratings yet
- EPLC Stage Gate Reviews Practices GuideDocument5 pagesEPLC Stage Gate Reviews Practices GuideAnonymous XgX8kTNo ratings yet
- Key Drug Information: RamiprilDocument1 pageKey Drug Information: Ramiprilamaliea234No ratings yet
- Unibis Leaflet EnglishDocument6 pagesUnibis Leaflet EnglishShna KawaNo ratings yet
- Defender 90 1993 1995 3.9L 4.2LDocument131 pagesDefender 90 1993 1995 3.9L 4.2LJuan QuispeNo ratings yet
- 327 - Mil-C-15074Document2 pages327 - Mil-C-15074Bianca MoraisNo ratings yet
- Cancer NursingDocument93 pagesCancer Nursingnursereview100% (2)
- Smart-Hydroponic-Based Framework For Saffron Cultivation: A Precision Smart Agriculture PerspectiveDocument19 pagesSmart-Hydroponic-Based Framework For Saffron Cultivation: A Precision Smart Agriculture PerspectiveTuấn Anh PhanNo ratings yet
- Memorial For RespondentDocument18 pagesMemorial For RespondentKandlagunta Gayathri PraharshithaNo ratings yet
- The Anxiety Sensitivity Index:: Construct Validity and Factor Analytic StructureDocument5 pagesThe Anxiety Sensitivity Index:: Construct Validity and Factor Analytic StructureTomás ArriazaNo ratings yet
- Unified Soil Classification Flowchart For Coarse-Grained SoilDocument7 pagesUnified Soil Classification Flowchart For Coarse-Grained SoilFraol TesfalemNo ratings yet
- Pze X5 enDocument6 pagesPze X5 enosiel limaNo ratings yet
- Chemistry Chapter 19 4ed Problems ScannedDocument18 pagesChemistry Chapter 19 4ed Problems ScannedeuniawapsNo ratings yet
- HPR6 12 Referencemanual EN 04RDocument40 pagesHPR6 12 Referencemanual EN 04RLUis FariaNo ratings yet
- Healthcare IT News July 2010Document40 pagesHealthcare IT News July 2010ChipNo ratings yet
- Available Scripts DetailsDocument8 pagesAvailable Scripts DetailsYogesh nNo ratings yet
- TranceDocument11 pagesTranceadeblarNo ratings yet
- Data Sheet - Provolt Dual Relay Multi-Tech Occupancy Sensor (O2C05 O2C10 O2C20-MDW)Document4 pagesData Sheet - Provolt Dual Relay Multi-Tech Occupancy Sensor (O2C05 O2C10 O2C20-MDW)Elkin Bautista RomeroNo ratings yet
- Smart Blind Stick Using ArduinoDocument4 pagesSmart Blind Stick Using ArduinoEditor IJTSRDNo ratings yet
- Community Development ProjectDocument15 pagesCommunity Development Projectabhi4you.lukNo ratings yet