You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Prospectus PDFDocument191 pagesProspectus PDFmekilis50% (4)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2 Octave Scales With Fingerings For Double BassDocument9 pages2 Octave Scales With Fingerings For Double BassFagner Magrinelli RochaNo ratings yet
- Saint-Saens Cello Concerto No1 PianoDocument23 pagesSaint-Saens Cello Concerto No1 PianoFagner Magrinelli RochaNo ratings yet
- Lalo 2 PDFDocument3 pagesLalo 2 PDFFagner Magrinelli RochaNo ratings yet
- Wohlfart Viola Etude 2 and 3Document1 pageWohlfart Viola Etude 2 and 3Fagner Magrinelli RochaNo ratings yet
- Joy To The World HarmoniesDocument15 pagesJoy To The World HarmoniesFagner Magrinelli RochaNo ratings yet
- Vivaldi G Minor Violin ConcertoDocument7 pagesVivaldi G Minor Violin ConcertoFagner Magrinelli RochaNo ratings yet
- Berlioz Hungarian MarchDocument21 pagesBerlioz Hungarian MarchFagner Magrinelli RochaNo ratings yet
- Handel - Violin Sonata in F MajorDocument19 pagesHandel - Violin Sonata in F MajorFagner Magrinelli Rocha100% (1)
- ASTA Why Strings Brochure IADocument2 pagesASTA Why Strings Brochure IAFagner Magrinelli RochaNo ratings yet
- Affinity Design in Action PDFDocument37 pagesAffinity Design in Action PDFFagner Magrinelli Rocha100% (6)
- Mozart Violin Sonata E Minor KV304 PianoDocument10 pagesMozart Violin Sonata E Minor KV304 PianoFagner Magrinelli RochaNo ratings yet
- 2014-2015 Academic Calendar: Classes Begin Aug. 25 Jan. 14 June 2 July 7Document1 page2014-2015 Academic Calendar: Classes Begin Aug. 25 Jan. 14 June 2 July 7Fagner Magrinelli RochaNo ratings yet
- Piazzolla FiveTangoSensationsDocument53 pagesPiazzolla FiveTangoSensationsGabrielaNo ratings yet
- Gabrieli Sonata PandF ScoreDocument11 pagesGabrieli Sonata PandF ScoreFagner Magrinelli RochaNo ratings yet
- OCDSB Secondary School Courses 2011-2012Document210 pagesOCDSB Secondary School Courses 2011-2012thelastdawnNo ratings yet
- Uttarakhand Board of Technical Education, Roorkee Semester /annual Examination-2021-22 (Winter) - New CourseDocument10 pagesUttarakhand Board of Technical Education, Roorkee Semester /annual Examination-2021-22 (Winter) - New CourseShubham RawatNo ratings yet
- 2015 2016 GRAD CatalogDocument722 pages2015 2016 GRAD CatalogAlexander León PuelloNo ratings yet
- DiplomaDocument18 pagesDiplomamanojkumarcnNo ratings yet
- Fees Structure For The 1st Year BE and ME Courses PDFDocument3 pagesFees Structure For The 1st Year BE and ME Courses PDFAtanuMajiNo ratings yet
- 11 IPD Graduate Guidelines FinalDocument12 pages11 IPD Graduate Guidelines FinalSrinivas SomasundaramNo ratings yet
- Course Curriculum Other ModalitiesDocument8 pagesCourse Curriculum Other ModalitiesRana NikeshNo ratings yet
- Syllabi 2020 Japanese Language Courses PDFDocument58 pagesSyllabi 2020 Japanese Language Courses PDF海狸No ratings yet
- MVG World History Syllabus Fall 2023-Spring 2024Document4 pagesMVG World History Syllabus Fall 2023-Spring 2024api-475618276No ratings yet
- ITECH Information BrochureDocument23 pagesITECH Information BrochureFauzan AlfiNo ratings yet
- Aps Student Calendar Sy24Document1 pageAps Student Calendar Sy24api-492684571No ratings yet
- Ewuundergraduate Bulletin 14th Edition Doc Version PDFDocument524 pagesEwuundergraduate Bulletin 14th Edition Doc Version PDFArman Husain100% (1)
- Academic Calendar 2018-19Document16 pagesAcademic Calendar 2018-19Ambuj AgrawalNo ratings yet
- ECN801 - Outline - W2015 - Sec 021Document5 pagesECN801 - Outline - W2015 - Sec 021Raunak TimilsinaNo ratings yet
- July August September: School Calendar 2017 - 2018Document1 pageJuly August September: School Calendar 2017 - 2018Juan ChavezNo ratings yet
- Academic Regulations B.Tech CSE PDFDocument138 pagesAcademic Regulations B.Tech CSE PDFabhiramNo ratings yet
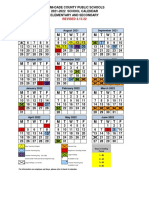
- FINAL MDCPS Elementary and Secondary Calendar 2021-2022Document2 pagesFINAL MDCPS Elementary and Secondary Calendar 2021-2022asdasdasdNo ratings yet
- Mahamaya Technical University, Noida: B. Tech. (Common For All Branches Except-Agricultural Engineering) Semester-IIDocument35 pagesMahamaya Technical University, Noida: B. Tech. (Common For All Branches Except-Agricultural Engineering) Semester-IIAshish RanjanNo ratings yet
- Course Outline: Option C: Scientific and Technical WritingDocument9 pagesCourse Outline: Option C: Scientific and Technical WritingAnthony BasantaNo ratings yet
- Kalender Akad 2021 RevisitedDocument1 pageKalender Akad 2021 Revisitedal hNo ratings yet
- PG Curriculum YearrDocument404 pagesPG Curriculum Yearrsubramanya1982No ratings yet
- 2019-April-UG-Rules+Policies+Curriculum+Syllabi-of-Courses 15 April 2019Document394 pages2019-April-UG-Rules+Policies+Curriculum+Syllabi-of-Courses 15 April 2019Prajwal MahajanNo ratings yet
- 2019 - 2020 Academic CalendarDocument3 pages2019 - 2020 Academic CalendarOlatundeNo ratings yet
- MoCU ALMANAC 2023-2024Document8 pagesMoCU ALMANAC 2023-2024othman HamzaNo ratings yet
- Info Eras 2021 DSTUTTGA01Document5 pagesInfo Eras 2021 DSTUTTGA01Lorenzo VivaldiNo ratings yet
- Lecturer Handbook 2019 - 2020: Office of The Provost Chapman UniversityDocument37 pagesLecturer Handbook 2019 - 2020: Office of The Provost Chapman UniversityTafadzwa KumaniNo ratings yet
- FORM Graduate Application For LOA 1Document1 pageFORM Graduate Application For LOA 1katbayogNo ratings yet
- Curricula Syllabi: M.TechDocument391 pagesCurricula Syllabi: M.TechY ANo ratings yet
- B. Tech Regular Four Year Degree Courses: Academic Regulations (R - 17) Course Structure AND Detailed SyllabiDocument73 pagesB. Tech Regular Four Year Degree Courses: Academic Regulations (R - 17) Course Structure AND Detailed SyllabifitsumNo ratings yet