You might also like
- Veterinary Surgical OncologyFrom EverandVeterinary Surgical OncologySimon T. KudnigNo ratings yet
- Certified Pediatric Emergency Nurse Review: Putting It All TogetherFrom EverandCertified Pediatric Emergency Nurse Review: Putting It All TogetherNo ratings yet
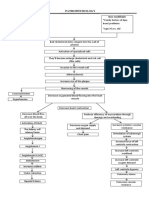
- Pathophysiology CHF MineDocument2 pagesPathophysiology CHF MineCalimlim KimNo ratings yet
- Working Phase (Psych Nursing) Progress Report Process ReportingDocument5 pagesWorking Phase (Psych Nursing) Progress Report Process ReportingCalimlim KimNo ratings yet
- Lab 8 - PWMDocument4 pagesLab 8 - PWMlol100% (1)
- Philippine Anti CyberbullyingDocument4 pagesPhilippine Anti CyberbullyingCalimlim Kim100% (2)
- News Portal Project ReportDocument34 pagesNews Portal Project ReportAbkash Khatua83% (12)
- A Practical Guide to Palliative Care in PaediatricsFrom EverandA Practical Guide to Palliative Care in PaediatricsRating: 5 out of 5 stars5/5 (1)
- Project Report Course Registration SystemDocument70 pagesProject Report Course Registration SystemImran Khan Mewati36% (14)
- Prelim Bioethics Handouts.Document13 pagesPrelim Bioethics Handouts.Calimlim KimNo ratings yet
- A Practical Guide to Palliative Care in Paediatrics: Paediatric Palliative Care for Health ProfessionalsFrom EverandA Practical Guide to Palliative Care in Paediatrics: Paediatric Palliative Care for Health ProfessionalsNo ratings yet
- Access the new Azure Portal and view subscription information in the dashboardDocument2 pagesAccess the new Azure Portal and view subscription information in the dashboardSaikrishNo ratings yet
- Disturbed Sensory PerceptionDocument3 pagesDisturbed Sensory PerceptionCalimlim Kim100% (1)
- PRC Form PDFDocument4 pagesPRC Form PDFShariff Bernardo SarikinNo ratings yet
- Cases Baby Vince NursingDocument5 pagesCases Baby Vince NursingSarah FabrosNo ratings yet
- PRC Form Cmo 14 IrishDocument6 pagesPRC Form Cmo 14 IrishJonathan ObañaNo ratings yet
- PRC 2Document5 pagesPRC 2Yendor Medalle PickeringNo ratings yet
- FINAL PRC Plain (Blank)Document6 pagesFINAL PRC Plain (Blank)Rez ApegoNo ratings yet
- PRC TinaDocument4 pagesPRC TinaCristina L. JaysonNo ratings yet
- Mindanao Sanitarium Nursing ClinicalsDocument1 pageMindanao Sanitarium Nursing ClinicalsCristina L. JaysonNo ratings yet
- Finalest of Them All!!!Document11 pagesFinalest of Them All!!!basinang_jangilNo ratings yet
- Sample PRC RequirementsDocument4 pagesSample PRC RequirementsRodney Beltran SubaranNo ratings yet
- CasesDocument6 pagesCasesDeck BinuyaNo ratings yet
- Max Suniel ST., Carmen, Cagayan de Oro CityDocument18 pagesMax Suniel ST., Carmen, Cagayan de Oro CityTinNo ratings yet
- Case KidotDocument7 pagesCase KidotcabantasNo ratings yet
- Medical Colleges of Northern PhillipinesDocument5 pagesMedical Colleges of Northern Phillipinesbarbiegirl9497No ratings yet
- PRC FormsDocument5 pagesPRC FormsKevinJanCelestinoNo ratings yet
- MemeDocument7 pagesMemeDiolan Novero BagorioNo ratings yet
- Golden Gate Colleges P. Prieto ST., Batangas CityDocument5 pagesGolden Gate Colleges P. Prieto ST., Batangas CityR ArcegaNo ratings yet
- Laguna Northwestern College: Patrick V. CalalangDocument1 pageLaguna Northwestern College: Patrick V. CalalangPat Vierneza-CalalangNo ratings yet
- PRCDocument6 pagesPRCKate ChavezNo ratings yet
- Case Slip DRDocument4 pagesCase Slip DRCalimlim KimNo ratings yet
- Roy Cord Dress DR in BRTTHDocument8 pagesRoy Cord Dress DR in BRTTHIbrahim RegachoNo ratings yet
- Or Case FormDocument2 pagesOr Case FormLovely Jane ArandaNo ratings yet
- PRC FormDocument6 pagesPRC FormKendraMargarethSerentasNo ratings yet
- UntitledDocument3 pagesUntitledapi-77115436No ratings yet
- CASES (Long Form)Document7 pagesCASES (Long Form)KiieEemNo ratings yet
- Amando Cope College College of Nursing: ODC Form 4Document2 pagesAmando Cope College College of Nursing: ODC Form 4Ibrahim RegachoNo ratings yet
- AfafnkDocument2 pagesAfafnkChris TianNo ratings yet
- Rose Cases FormDocument2 pagesRose Cases FormRose Ann GutierrezNo ratings yet
- CasesDocument3 pagesCasesBeGie MamBaNo ratings yet
- PRCDocument10 pagesPRCKatie TenebroNo ratings yet
- PRC Form Ralph NewaaaaaaaaaaaaaaaaaaaaaDocument13 pagesPRC Form Ralph NewaaaaaaaaaaaaaaaaaaaaaJabez TyNo ratings yet
- Palasol 7 (Final)Document6 pagesPalasol 7 (Final)Afreah BebzNo ratings yet
- Western Mindanao State UniversityDocument4 pagesWestern Mindanao State UniversityJehannaMarEnggingAbdurahmanNo ratings yet
- NewbornDocument4 pagesNewbornRI NANo ratings yet
- Wfmc-Camarin Sample - DR Actual - Assist.cordcare PRC FormsDocument4 pagesWfmc-Camarin Sample - DR Actual - Assist.cordcare PRC FormsNes TiiNo ratings yet
- St. Anthony College of Roxas City, Inc.: Noted By: Approved By: Clinical Coordinator, PRC I.D Dean, PRC I.DDocument6 pagesSt. Anthony College of Roxas City, Inc.: Noted By: Approved By: Clinical Coordinator, PRC I.D Dean, PRC I.DShoixi ⎝⓿⏝⓿⎠No ratings yet
- ORDocument20 pagesORTrish AldonNo ratings yet
- WMSU Nursing FormsDocument4 pagesWMSU Nursing FormsreraysNo ratings yet
- Resume KyleGolindang RevisedDocument6 pagesResume KyleGolindang RevisedKylie GolindangNo ratings yet
- MELVYNDocument6 pagesMELVYNJohnedel RosalesNo ratings yet
- University of Pangasinan College of Nursing: Minor OperationDocument6 pagesUniversity of Pangasinan College of Nursing: Minor OperationJohnedel RosalesNo ratings yet
- PCC Nursing FormsDocument6 pagesPCC Nursing Formsthomasfinley44No ratings yet
- DAMES OR Templates EVMCDocument3 pagesDAMES OR Templates EVMCJamie John EsplanadaNo ratings yet
- "The Institution For Better Life": Northern Christian College College of NursingDocument5 pages"The Institution For Better Life": Northern Christian College College of NursingMorayata AlishabulaNo ratings yet
- I. Major Operations: Urdaneta City UniversityDocument11 pagesI. Major Operations: Urdaneta City UniversityEdgar GarciaNo ratings yet
- Brent Hospital and Colleges IncorporatedDocument4 pagesBrent Hospital and Colleges IncorporatedAlessandra MoonNo ratings yet
- Dalman 222Document7 pagesDalman 222Cyril D. SuazoNo ratings yet
- Sheryl Ann B. Pedines: The Institution For Better LifeDocument4 pagesSheryl Ann B. Pedines: The Institution For Better LifeSheryl Ann Barit PedinesNo ratings yet
- PRC LeahDocument8 pagesPRC LeahInes Hamoy JunioNo ratings yet
- ODC Form 3 - Assisted Delivery RecordDocument1 pageODC Form 3 - Assisted Delivery RecordIbrahim RegachoNo ratings yet
- PRC Form CasesDocument5 pagesPRC Form CasesAyen Fajardo-HernalNo ratings yet
- Minor or Format TemplateDocument2 pagesMinor or Format TemplateKwesi YasayNo ratings yet
- Mark ExhibitDocument8 pagesMark ExhibitRichard281981No ratings yet
- Bukidnon State University: DR ActualDocument1 pageBukidnon State University: DR ActualKryza Dale Bunado BaticanNo ratings yet
- TemplatesDocument5 pagesTemplatesLeon Darny Tahud PradiaNo ratings yet
- Disaster Preparedness for Healthcare FacilitiesFrom EverandDisaster Preparedness for Healthcare FacilitiesRating: 2 out of 5 stars2/5 (3)
- Introduction Brain Abcess Nursing ManagementDocument2 pagesIntroduction Brain Abcess Nursing ManagementCalimlim KimNo ratings yet
- Why Study A Masters in Surgical Nursing?Document5 pagesWhy Study A Masters in Surgical Nursing?Calimlim KimNo ratings yet
- Red Cross 143 Program 3Document23 pagesRed Cross 143 Program 3Calimlim KimNo ratings yet
- Path o Physiology GastrroDocument1 pagePath o Physiology GastrroCalimlim KimNo ratings yet
- NCPsDocument11 pagesNCPsCalimlim KimNo ratings yet
- Understanding Breast DisordersDocument13 pagesUnderstanding Breast DisordersCalimlim KimNo ratings yet
- How to open a password protected zip fileDocument2 pagesHow to open a password protected zip fileSumber UnduhNo ratings yet
- NursingDocument4 pagesNursingCalimlim KimNo ratings yet
- Bioethics Assignment 1Document2 pagesBioethics Assignment 1Calimlim KimNo ratings yet
- Sal But AmolDocument2 pagesSal But AmolCalimlim KimNo ratings yet
- Bioethics Assignment 1Document2 pagesBioethics Assignment 1Calimlim KimNo ratings yet
- The Importance of SanitationDocument3 pagesThe Importance of SanitationCalimlim KimNo ratings yet
- Case SlipDocument4 pagesCase SlipCalimlim KimNo ratings yet
- Effects of Social Media on Nurses' Work PerformanceDocument42 pagesEffects of Social Media on Nurses' Work PerformanceCalimlim Kim100% (1)
- Chapter 18Document34 pagesChapter 18Calimlim KimNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationCalimlim KimNo ratings yet
- Lnu Case SlipDocument4 pagesLnu Case SlipCalimlim KimNo ratings yet
- CSR AppDocument2 pagesCSR AppCalimlim KimNo ratings yet
- A Novel Mouse Model of High FlowDocument1 pageA Novel Mouse Model of High FlowCalimlim KimNo ratings yet
- Late Onset Asthma & Cardiovascular Disease RisksDocument2 pagesLate Onset Asthma & Cardiovascular Disease RisksCalimlim KimNo ratings yet
- Case PresentationDocument55 pagesCase PresentationCalimlim KimNo ratings yet
- Case Slip DRDocument4 pagesCase Slip DRCalimlim KimNo ratings yet
- FINAL Discharge-PlanningDocument3 pagesFINAL Discharge-PlanningCalimlim KimNo ratings yet
- Laboratory Result SampleDocument2 pagesLaboratory Result SampleCalimlim KimNo ratings yet
- Dumping Syndrome 508Document8 pagesDumping Syndrome 508Calimlim KimNo ratings yet
- INF1511 MemoDocument3 pagesINF1511 Memoclaudz100% (1)
- Content:: Galileo Reissue/ExchangeDocument10 pagesContent:: Galileo Reissue/ExchangeNeomi SaneNo ratings yet
- Consolidated Changes For 59 The DitionDocument613 pagesConsolidated Changes For 59 The DitionSHERIEFNo ratings yet
- Composer Firmware Updater InstructionsDocument5 pagesComposer Firmware Updater InstructionsMulyana AhmadNo ratings yet
- C++ Lab MaualDocument89 pagesC++ Lab MaualRajat KumarNo ratings yet
- Burnes 2004Document18 pagesBurnes 2004Asmadera Mat EsaNo ratings yet
- Experian Dispute FormDocument1 pageExperian Dispute Formmainester100% (3)
- Anup Kumar Gupta-Microsoft Certified Professional ResumeDocument4 pagesAnup Kumar Gupta-Microsoft Certified Professional ResumeAnup kumar GuptaNo ratings yet
- Origin C Programming GuideDocument287 pagesOrigin C Programming GuideRaviranjan Kumar SinghNo ratings yet
- How to setup Bristol Audio Synthesis with 64 StudioDocument5 pagesHow to setup Bristol Audio Synthesis with 64 StudiobobmeanzaNo ratings yet
- 1 IdnDocument2 pages1 IdnmohanapriyaNo ratings yet
- TolAnalyst TutorialDocument15 pagesTolAnalyst TutorialAnton Nanchev100% (1)
- Analog Laboratory enDocument82 pagesAnalog Laboratory enAud IoirdNo ratings yet
- Transactional Licensing Comparison ChartDocument3 pagesTransactional Licensing Comparison Chartjonder2000No ratings yet
- Johnson's Algorithm For Optimal Scheduling Of Multi-Machine SystemsDocument8 pagesJohnson's Algorithm For Optimal Scheduling Of Multi-Machine SystemsBabyCoder HvhNo ratings yet
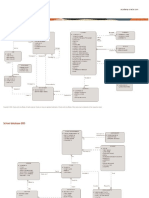
- PLSQL Schema ERD and Table DesignsDocument8 pagesPLSQL Schema ERD and Table DesignsSoham GholapNo ratings yet
- IT Problem Management SOPDocument9 pagesIT Problem Management SOPNova SetyaningrumNo ratings yet
- MS HandoutDocument3 pagesMS HandoutJayant JawanjalNo ratings yet
- Mom PDFDocument8 pagesMom PDFThug LifeNo ratings yet
- Dxdiag LumionDocument49 pagesDxdiag Lumionrahmat nurfitriantoNo ratings yet
- GMCC GPRS & EDGE RADIO KPI DASHBOARDDocument18 pagesGMCC GPRS & EDGE RADIO KPI DASHBOARDyousef shabanNo ratings yet
- Magic 3d Easy View Manual Es PDFDocument32 pagesMagic 3d Easy View Manual Es PDFAngel Santiago Silva HuamalianoNo ratings yet
- Scan APIDocument183 pagesScan APIChitradeep Dutta RoyNo ratings yet
- Guide For Interface Developers: Everything You Need To Know About Energyplus Input and OutputDocument33 pagesGuide For Interface Developers: Everything You Need To Know About Energyplus Input and OutputWormInchNo ratings yet
- Install, 1Document18 pagesInstall, 1PetzyMarianNo ratings yet
- Key Office 2013Document4 pagesKey Office 2013Mas GunawanNo ratings yet