You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Wbs and Division of Work Excel Spread Sheet1Document12 pagesWbs and Division of Work Excel Spread Sheet1Adrian Christian Lee100% (1)
- Recent Advances in Obstetrics & Gynecology Volume 21Document201 pagesRecent Advances in Obstetrics & Gynecology Volume 21Fajar Ahmad Prasetya77% (13)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Uji Aktivitas Antimikroba Ekstrak Cabai Rawit (CapsicumDocument19 pagesUji Aktivitas Antimikroba Ekstrak Cabai Rawit (CapsicumTri RatnawatiNo ratings yet
- And Metalloprotease-33), Gen Yang Ditemukan Pada Tahun 2002. Selain FaktorDocument3 pagesAnd Metalloprotease-33), Gen Yang Ditemukan Pada Tahun 2002. Selain FaktorTri RatnawatiNo ratings yet
- Matrikulasi MM-Kaligawe 27 Nop 2012Document26 pagesMatrikulasi MM-Kaligawe 27 Nop 2012Tri RatnawatiNo ratings yet
- Lymphocytes in Schizophrenic Patients Under Therapy: Serological, Morphological and Cell Subset FindingsDocument1 pageLymphocytes in Schizophrenic Patients Under Therapy: Serological, Morphological and Cell Subset FindingsTri RatnawatiNo ratings yet
- Anestesi RegionalDocument41 pagesAnestesi RegionalTri RatnawatiNo ratings yet
- Procedure For DefibrillationDocument6 pagesProcedure For DefibrillationTri RatnawatiNo ratings yet
- Shockable and Unshockable RhytmDocument8 pagesShockable and Unshockable RhytmTri RatnawatiNo ratings yet
- Pomfoliks JurnalDocument4 pagesPomfoliks JurnalTri RatnawatiNo ratings yet
- Primitive Reflexes and Postural Reactions in The Neurodevelopmental ExaminationDocument8 pagesPrimitive Reflexes and Postural Reactions in The Neurodevelopmental ExaminationTri RatnawatiNo ratings yet
- EYE Emergency Manual An Illustrated Guide: Second EditionDocument51 pagesEYE Emergency Manual An Illustrated Guide: Second EditionMin MawNo ratings yet
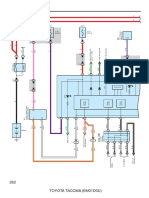
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- Condition Montoring of TransformerDocument0 pagesCondition Montoring of TransformerDevansh SinghNo ratings yet
- ElectronicsDocument6 pagesElectronicsAayush AgrawalNo ratings yet
- Proline Promass 83 Profibus Dp/Pa: Description of Device FunctionsDocument182 pagesProline Promass 83 Profibus Dp/Pa: Description of Device FunctionsHectorNo ratings yet
- A Bank Is A Financial Institution That Serves As A Financial IntermediaryDocument12 pagesA Bank Is A Financial Institution That Serves As A Financial IntermediaryShubhankar SoniNo ratings yet
- Call For Papers-International Journal of Wireless & Mobile Networks (IJWMN)Document2 pagesCall For Papers-International Journal of Wireless & Mobile Networks (IJWMN)John BergNo ratings yet
- FUFENG-AF 80 Xanthan Gum SDSDocument6 pagesFUFENG-AF 80 Xanthan Gum SDSDheyne TellesNo ratings yet
- Guwahati Conference Circular 1Document5 pagesGuwahati Conference Circular 1Phyoben S OdyuoNo ratings yet
- I. Preparation: Lesson 2 Concept of Ecosystem Intended Learning OutcomeDocument17 pagesI. Preparation: Lesson 2 Concept of Ecosystem Intended Learning OutcomeLeslie ObisoNo ratings yet
- Phontech Ics 6200Document193 pagesPhontech Ics 6200danh voNo ratings yet
- Near Field Communication Based College CanteenDocument5 pagesNear Field Communication Based College CanteenJunaid M FaisalNo ratings yet
- Erd 2 F 005Document1 pageErd 2 F 005Bettina BarrionNo ratings yet
- DOT Hazmat Training For Nuclear Medicine Technologists - Rules of The RoadDocument50 pagesDOT Hazmat Training For Nuclear Medicine Technologists - Rules of The RoadAdji Achmad J BramantyaNo ratings yet
- Read The Text Carefully and Then Answer The Questions That Follow! Floods Force Thousands of People To Evacuate in GorontaloDocument2 pagesRead The Text Carefully and Then Answer The Questions That Follow! Floods Force Thousands of People To Evacuate in GorontaloDella SagitaNo ratings yet
- Principles of Christian Mental HealthDocument27 pagesPrinciples of Christian Mental HealthMaschil100% (2)
- This Study Resource Was: Pas 41 - AgricultureDocument3 pagesThis Study Resource Was: Pas 41 - Agriculturedasha limNo ratings yet
- Risk Assessment: Construction Plan For Box Girder Joints, Wing Plates and Anti-Collision GuardrailsDocument3 pagesRisk Assessment: Construction Plan For Box Girder Joints, Wing Plates and Anti-Collision Guardrailssalauddin0mohammedNo ratings yet
- Nuccore ResultDocument2,189 pagesNuccore ResultJohanS.Acebedo0% (1)
- Methane Recovery Project - Final PDFDocument18 pagesMethane Recovery Project - Final PDFZayin ValerieNo ratings yet
- Evap-Lt 60 KV CG ShimaDocument439 pagesEvap-Lt 60 KV CG ShimaDax CasraNo ratings yet
- Cadôr - Books About Nothing PDFDocument4 pagesCadôr - Books About Nothing PDFFelipeCussen100% (1)
- MANUALESDocument84 pagesMANUALESPedroJose0% (1)
- COVID 19 PP Original 1Document20 pagesCOVID 19 PP Original 1Anthony UjeneNo ratings yet
- Writing A Literary Essay - 3Document10 pagesWriting A Literary Essay - 3Yilia WangNo ratings yet
- University of Waterloo Department of Mechanical Engineering ME524 - Advanced Dynamics Adams Tutorial 1 Winter 2007 ObjectiveDocument10 pagesUniversity of Waterloo Department of Mechanical Engineering ME524 - Advanced Dynamics Adams Tutorial 1 Winter 2007 Objectivemass1981No ratings yet
- 1 - Aqueduct RETROSPECTOSDocument10 pages1 - Aqueduct RETROSPECTOSirving.barrios.vzlaNo ratings yet
- Theories of International TradeDocument11 pagesTheories of International Tradeesha bansalNo ratings yet
- Unit 4 Notes GDJPDocument2 pagesUnit 4 Notes GDJPAnanth VelNo ratings yet