You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ALERT Lays Charges Against 11 People Following Drug-Trafficking InvestigationDocument1 pageALERT Lays Charges Against 11 People Following Drug-Trafficking InvestigationAnonymous NbMQ9YmqNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Finding Your Own Fountain of Youth - Andrew SiegelDocument242 pagesFinding Your Own Fountain of Youth - Andrew Siegelnotedddd100% (1)
- Nurse practitioners provide healthcare beyond RN scopeDocument6 pagesNurse practitioners provide healthcare beyond RN scopeJakeGilNo ratings yet
- Principles and Practice of Endocrinology and MetabolismDocument1,784 pagesPrinciples and Practice of Endocrinology and MetabolismNovian Abadi75% (4)
- Kerala Health PolicyDocument31 pagesKerala Health PolicyanukeralaNo ratings yet
- Liabilities of HospitalsDocument36 pagesLiabilities of HospitalsMJ Carreon100% (1)
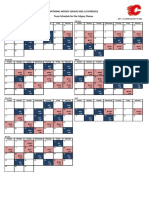
- Calgary Flames 2022-23 ScheduleDocument2 pagesCalgary Flames 2022-23 ScheduleAnonymous NbMQ9YmqNo ratings yet
- Saima Jamal's Letter To Calgary Police, Councillors and Mayor Jyoti GondekDocument2 pagesSaima Jamal's Letter To Calgary Police, Councillors and Mayor Jyoti GondekAnonymous NbMQ9YmqNo ratings yet
- Letter To Calgary PrideDocument2 pagesLetter To Calgary PrideAnonymous NbMQ9Ymq100% (1)
- Ray Jones' Retirement LetterDocument1 pageRay Jones' Retirement LetterAnonymous NbMQ9YmqNo ratings yet
- Policy and Statement of ATA in Support of Vaccine MandateDocument2 pagesPolicy and Statement of ATA in Support of Vaccine MandateAnonymous NbMQ9YmqNo ratings yet
- LRT Transit PrioritiesDocument6 pagesLRT Transit PrioritiesAnonymous NbMQ9YmqNo ratings yet
- Eye On Alberta - Alberta's Public Affairs Monitor - March 2022Document7 pagesEye On Alberta - Alberta's Public Affairs Monitor - March 2022Anonymous NbMQ9YmqNo ratings yet
- Guidance For Professional Sporting TournamentsDocument3 pagesGuidance For Professional Sporting TournamentsAnonymous NbMQ9YmqNo ratings yet
- Edmonton Police Association LetterDocument3 pagesEdmonton Police Association LetterCTV News EdmontonNo ratings yet
- S&P Rating Report For City of EdmontonDocument7 pagesS&P Rating Report For City of EdmontonAnonymous NbMQ9YmqNo ratings yet
- Final - Notice of Motion - Advocating For Creation of Task Force On Property Tax Assessment ReformDocument2 pagesFinal - Notice of Motion - Advocating For Creation of Task Force On Property Tax Assessment ReformAnonymous NbMQ9YmqNo ratings yet
- May 13 2020 Gary Bettman NHLDocument2 pagesMay 13 2020 Gary Bettman NHLAnonymous NbMQ9YmqNo ratings yet
- Aha Letter To Alberta Governement - Jan 13Document2 pagesAha Letter To Alberta Governement - Jan 13Anonymous NbMQ9YmqNo ratings yet
- Outdoor Stores Letter To Alberta Government About Parks ClosuresDocument1 pageOutdoor Stores Letter To Alberta Government About Parks ClosuresAnonymous NbMQ9YmqNo ratings yet
- Alberta Court of Appeal Document On Prosper's Rigel Oilsands ProjectDocument10 pagesAlberta Court of Appeal Document On Prosper's Rigel Oilsands ProjectAnonymous NbMQ9YmqNo ratings yet
- Physicians For Alberta HealthcareDocument11 pagesPhysicians For Alberta HealthcareAnonymous NbMQ9YmqNo ratings yet
- Alberta Seclusion Room JudgmentDocument7 pagesAlberta Seclusion Room JudgmentAnonymous NbMQ9YmqNo ratings yet
- 2020 02 18 Environics - Alberta Teacher Assoc Survey Dec 19Document8 pages2020 02 18 Environics - Alberta Teacher Assoc Survey Dec 19Anonymous NbMQ9YmqNo ratings yet
- Letter To AHS CEODocument2 pagesLetter To AHS CEOAnonymous NbMQ9YmqNo ratings yet
- AMA Letter On Bill 207Document1 pageAMA Letter On Bill 207Anonymous NbMQ9YmqNo ratings yet
- Letter To Federal Government From Doug SchweitzerDocument2 pagesLetter To Federal Government From Doug SchweitzerAnonymous NbMQ9YmqNo ratings yet
- Statement by Integrity Commissioner Sal J. LoVecchioDocument1 pageStatement by Integrity Commissioner Sal J. LoVecchioAnonymous NbMQ9YmqNo ratings yet
- Fort McKay First Nation Statement On Prosper Petroleum Ltd. CaseDocument2 pagesFort McKay First Nation Statement On Prosper Petroleum Ltd. CaseAnonymous NbMQ9YmqNo ratings yet
- Final - Notice of Motion - Advocating For Creation of Task Force On Property Tax Assessment ReformDocument2 pagesFinal - Notice of Motion - Advocating For Creation of Task Force On Property Tax Assessment ReformAnonymous NbMQ9YmqNo ratings yet
- Injunction Granted in Dispute Over POWER 107 NameDocument20 pagesInjunction Granted in Dispute Over POWER 107 NameAnonymous NbMQ9YmqNo ratings yet
- Obesity Canada InfographicDocument1 pageObesity Canada InfographicAnonymous NbMQ9YmqNo ratings yet
- Holiday Turkey Sheet (Graphics)Document2 pagesHoliday Turkey Sheet (Graphics)Anonymous NbMQ9YmqNo ratings yet
- U of C Graduate Students' Association Tuition Increase Protest LetterDocument3 pagesU of C Graduate Students' Association Tuition Increase Protest LetterCTV CalgaryNo ratings yet
- AMA Letter About Bill 207Document1 pageAMA Letter About Bill 207Anonymous NbMQ9YmqNo ratings yet
- Minnesota's Health Care WorkforceDocument8 pagesMinnesota's Health Care WorkforceinforumdocsNo ratings yet
- 2022 Member Brochure EvolveDocument28 pages2022 Member Brochure EvolveMagdomkakNo ratings yet
- Medical Economics Magazine PDFDocument41 pagesMedical Economics Magazine PDFxtineNo ratings yet
- Medical Document Authorizing The Use of Cannabis For Medical Purposes Under The Access To Cannabis For Medical Purposes RegulationsDocument2 pagesMedical Document Authorizing The Use of Cannabis For Medical Purposes Under The Access To Cannabis For Medical Purposes RegulationsAm MNo ratings yet
- Gujarat Civil Services Rules SummaryDocument51 pagesGujarat Civil Services Rules SummaryRitunjay JhaNo ratings yet
- To Work in Emergency Medical FieldDocument2 pagesTo Work in Emergency Medical FieldDr. Afsana NawheenNo ratings yet
- Indonesia Health Profile 2015 HighlightsDocument416 pagesIndonesia Health Profile 2015 Highlightssgd 2No ratings yet
- ABFM LetterDocument1 pageABFM LetterTadao Okada, MD, MPH, DABFM, FAAFPNo ratings yet
- The Church: Medical Centre: "The Church Is Not A Museum of Saints, But A Hospital For Sinners."Document4 pagesThe Church: Medical Centre: "The Church Is Not A Museum of Saints, But A Hospital For Sinners."Jada FennellNo ratings yet
- Perceptions of Government Hospital ServicesDocument7 pagesPerceptions of Government Hospital Servicesrokeya tamannaNo ratings yet
- Brochure Temple OrthoSymposium2018 ADocument5 pagesBrochure Temple OrthoSymposium2018 Ayos_peace86No ratings yet
- Code of Ethics For DoctorsDocument19 pagesCode of Ethics For DoctorsRealee AgustinNo ratings yet
- SCOPE Student's HandbookDocument15 pagesSCOPE Student's HandbookzmogasNo ratings yet
- Application Form For Permanent RegistrationDocument6 pagesApplication Form For Permanent Registrationtejbirsingh2013No ratings yet
- Carcedo Vs Maine MarineDocument18 pagesCarcedo Vs Maine MarineChristian Marko CabahugNo ratings yet
- Subject: Sample Outcomes-Based Curriculum For The Doctor of Optometry ProgramDocument18 pagesSubject: Sample Outcomes-Based Curriculum For The Doctor of Optometry ProgramJay R DomrigueNo ratings yet
- DBMS Assignment 1Document3 pagesDBMS Assignment 1Manu Garg100% (1)
- LECTURE 2: Organon 2 The Highest Ideal of A CureDocument8 pagesLECTURE 2: Organon 2 The Highest Ideal of A CureOana SandraNo ratings yet
- My First Visit To KosovaDocument10 pagesMy First Visit To KosovaFjala e LireNo ratings yet
- The Filipino Physician and EldsDocument13 pagesThe Filipino Physician and EldsYel AdreNo ratings yet
- Wa0012.Document49 pagesWa0012.Subho OfficialNo ratings yet
- Here Are 3 Benefits of Healthcare MarketingDocument3 pagesHere Are 3 Benefits of Healthcare MarketingCIO Advisor ApacNo ratings yet
- Wilfred Anderson 1 PDFDocument83 pagesWilfred Anderson 1 PDFWKYC.comNo ratings yet
- Focus 2 Combined Assessments 4593229Document6 pagesFocus 2 Combined Assessments 4593229Araceli HernandezNo ratings yet
- HLTH 101 Research PaperDocument9 pagesHLTH 101 Research Paperapi-625678417No ratings yet