You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- 9 Types of Female Orgasms ExplainedDocument4 pages9 Types of Female Orgasms ExplainedAbdul SyukurNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Vitamin Water - Arnel Ricafranca PDFDocument32 pagesVitamin Water - Arnel Ricafranca PDFAlaa EssamNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Musculoskeletal Physical TherapyDocument5 pagesMusculoskeletal Physical TherapyAbiha AnisNo ratings yet
- Small-Sided Games and Integrating Physical PreparationDocument196 pagesSmall-Sided Games and Integrating Physical Preparationbolebs1475% (4)
- NCM 101 Vital Signs PPT BSN 1a Group 1Document138 pagesNCM 101 Vital Signs PPT BSN 1a Group 1Brian Anthony100% (1)
- Can Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.Document15 pagesCan Mindfulness in Health Care Professionals Improve Patient Care An Integrative Review and Proposed Model.ALIXNo ratings yet
- Top 10 Graphic Design Interview Questions and AnswersDocument16 pagesTop 10 Graphic Design Interview Questions and Answersbetsjonh100% (1)
- Professional Growth and DevelopmentDocument154 pagesProfessional Growth and DevelopmentNina Anne Paracad100% (3)
- Grizz Phys Tier 2 PDFDocument19 pagesGrizz Phys Tier 2 PDFJ VivianNo ratings yet
- Study To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaDocument59 pagesStudy To Access The Knowledge Under Five Mothers Regarding Prevention of Malnutrition in Ankuli Berhampur Ganjam OdishaPabhat Kumar100% (2)
- Rotator Cuff StudyDocument8 pagesRotator Cuff StudyVivek Agrawal MDNo ratings yet
- Arthroscopic Decompression of A Bony Suprascapular Foramen: Technical NoteDocument4 pagesArthroscopic Decompression of A Bony Suprascapular Foramen: Technical NoteVivek Agrawal MDNo ratings yet
- Rotator Cuff RepairDocument3 pagesRotator Cuff RepairVivek Agrawal MDNo ratings yet
- Rotator Cuff RepairDocument3 pagesRotator Cuff RepairVivek Agrawal MDNo ratings yet
- AC Shoulder DislocationDocument8 pagesAC Shoulder DislocationVivek Agrawal MDNo ratings yet
- Rotator Cuff StudyDocument8 pagesRotator Cuff StudyVivek Agrawal MDNo ratings yet
- Arthroscopic Decompression of A Bony Suprascapular Foramen: Technical NoteDocument4 pagesArthroscopic Decompression of A Bony Suprascapular Foramen: Technical NoteVivek Agrawal MDNo ratings yet
- AC Shoulder DislocationDocument8 pagesAC Shoulder DislocationVivek Agrawal MDNo ratings yet
- AC Shoulder DislocationDocument5 pagesAC Shoulder DislocationVivek Agrawal MDNo ratings yet
- Rotator Cuff Repair StudyDocument7 pagesRotator Cuff Repair StudyVivek Agrawal MDNo ratings yet
- Rotator Cuff StudyDocument8 pagesRotator Cuff StudyVivek Agrawal MDNo ratings yet
- Frozen ShoulderDocument1 pageFrozen ShoulderVivek Agrawal MDNo ratings yet
- Arthroscopic Rotator Cuff Repair ProtocolDocument70 pagesArthroscopic Rotator Cuff Repair ProtocolVivek Agrawal MDNo ratings yet
- Arthroscopic Rotator Cuff Repair ProtocolDocument3 pagesArthroscopic Rotator Cuff Repair ProtocolVivek Agrawal MDNo ratings yet
- Total Shoulder ArthroplastyDocument3 pagesTotal Shoulder ArthroplastyVivek Agrawal MDNo ratings yet
- Reverse Total Shoulder ProtocolDocument2 pagesReverse Total Shoulder Protocolsurender_singh_43No ratings yet
- Pinched Nerve ShoulderDocument4 pagesPinched Nerve ShoulderVivek Agrawal MDNo ratings yet
- Rotator Cuff RepairDocument3 pagesRotator Cuff RepairVivek Agrawal MDNo ratings yet
- Shoulder Replacement ProtocolDocument2 pagesShoulder Replacement ProtocolVivek Agrawal MDNo ratings yet
- Appendix7 I-131Document4 pagesAppendix7 I-131Crizzz001No ratings yet
- Organon of Medicine All Years 2marks Question Viva Questions AnswersDocument12 pagesOrganon of Medicine All Years 2marks Question Viva Questions Answersabcxyz15021999No ratings yet
- Que No4 & 5-With Clues and Without CluesDocument4 pagesQue No4 & 5-With Clues and Without CluesMir Yamin Uddin ZidanNo ratings yet
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- Live deer placenta stem cells not found in food supplement capsulesDocument1 pageLive deer placenta stem cells not found in food supplement capsulesJohn LêNo ratings yet
- Causes of Baby Dumping: Family Breakups, Lack of Education, and PovertyDocument2 pagesCauses of Baby Dumping: Family Breakups, Lack of Education, and Povertysirthana697547No ratings yet
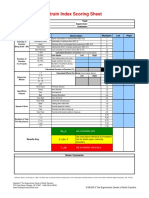
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- ResistanceDocument8 pagesResistanceAndi Soraya WalyddainiNo ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- Borderline Personality DisorderDocument7 pagesBorderline Personality DisorderleaNo ratings yet
- OBG ChapterDocument3 pagesOBG ChapterMohd IrfanNo ratings yet
- POne MPFFL 7 RV VPSX LQRPDocument3 pagesPOne MPFFL 7 RV VPSX LQRPRavi KumarNo ratings yet
- Improving Security of United Nations Peacekeepers ReportDocument43 pagesImproving Security of United Nations Peacekeepers Reportnelson duringNo ratings yet
- Pathology of the EndocardiumDocument31 pagesPathology of the EndocardiumAlexe VladNo ratings yet
- ICICI Bank Mortgage - HS360 Product FinalDocument29 pagesICICI Bank Mortgage - HS360 Product FinalRishu GiriNo ratings yet
- Affidavit of Accident Dominador Rosario BagamaspadDocument2 pagesAffidavit of Accident Dominador Rosario BagamaspadJaime GonzalesNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- High Birth Rate Is A Special Feature of All The Developing EconomiesDocument3 pagesHigh Birth Rate Is A Special Feature of All The Developing EconomiesMuhammad SohaibNo ratings yet
- TWC Final Settlement DocsDocument374 pagesTWC Final Settlement DocsTHROnlineNo ratings yet