You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Afib NCPDocument3 pagesAfib NCPGen RodriguezNo ratings yet
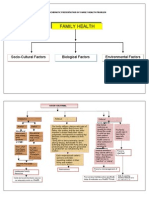
- Family Health: Socio-Cultural Factors Biological Factors Environmental FactorsDocument16 pagesFamily Health: Socio-Cultural Factors Biological Factors Environmental FactorsFritz Regis W. TumaponNo ratings yet
- Chest Tube ThoracostomyDocument1 pageChest Tube ThoracostomyFritz Regis W. TumaponNo ratings yet
- ER DRUGS AT A GLANCEDocument3 pagesER DRUGS AT A GLANCEmyleneacar100% (3)
- Table of ContentDocument2 pagesTable of ContentFritz Regis W. TumaponNo ratings yet
- BCU Edit Tomat PDFDocument16 pagesBCU Edit Tomat PDFmuhammad adamNo ratings yet
- Cardiac Tamponade: An Educational Review: Massimo Imazio and Gaetano Maria de FerrariDocument9 pagesCardiac Tamponade: An Educational Review: Massimo Imazio and Gaetano Maria de FerrariAngela OrozcoNo ratings yet
- Cardiac TamponadeDocument2 pagesCardiac TamponadechoobiNo ratings yet
- Lapsus + CHF CAD AbcDocument41 pagesLapsus + CHF CAD AbcMiftah Farid AsmaunNo ratings yet
- Clubbing Amd Myo InfracDocument7 pagesClubbing Amd Myo InfracokaciaNo ratings yet
- Manage Cardiac Output in Hyperthyroid PatientDocument3 pagesManage Cardiac Output in Hyperthyroid PatientPrincess QuirinaNo ratings yet
- BPS Board Certified Cardiology Syllabus For Entrance ExamDocument5 pagesBPS Board Certified Cardiology Syllabus For Entrance ExamGHAPRC RUDRAPURNo ratings yet
- Physio Control Lifepak 12 Operating Instructions 2Document187 pagesPhysio Control Lifepak 12 Operating Instructions 2A. A.G.No ratings yet
- Vijayalakshmi 2008Document7 pagesVijayalakshmi 2008Rakesh DashNo ratings yet
- Echocardiography Curriculum ToolDocument11 pagesEchocardiography Curriculum ToolJoseph BarkerNo ratings yet
- iFR Vs FFR For Guiding Coronary Revascularization - DEFINE-FLAIR (2 Year Results)Document32 pagesiFR Vs FFR For Guiding Coronary Revascularization - DEFINE-FLAIR (2 Year Results)rainmed USNo ratings yet
- Morgan 2012Document5 pagesMorgan 2012aixacamila3No ratings yet
- EHealth and COVIDDocument10 pagesEHealth and COVIDWalter ReyesNo ratings yet
- Nursing Care Plan AnswerDocument6 pagesNursing Care Plan Answercoosa liquorsNo ratings yet
- Pharmacology of Antiarrhythmic Drugs - RecordedDocument33 pagesPharmacology of Antiarrhythmic Drugs - RecordedSarah SabtiNo ratings yet
- Acute Coronary SyndromeDocument24 pagesAcute Coronary SyndromeMuhammad Alauddin Sarwar100% (8)
- Differences BTW ACS, Stable AnginaDocument7 pagesDifferences BTW ACS, Stable AnginaCarmenhNo ratings yet
- Tetralogy of Fallot: Cyanotic Congenital Heart DiseaseDocument31 pagesTetralogy of Fallot: Cyanotic Congenital Heart DiseaseJabir EspinaNo ratings yet
- Valvular Heart Diseases & CardiomyopathiesDocument73 pagesValvular Heart Diseases & CardiomyopathiesDammaqsaa W BiyyanaaNo ratings yet
- Cardiac DiseasesDocument8 pagesCardiac DiseasesTJ NgNo ratings yet
- Prometric McqsDocument30 pagesPrometric Mcqsjishan8250% (2)
- Ic Guía Esc 2021-99-128Document30 pagesIc Guía Esc 2021-99-128aassNo ratings yet
- 2023 Food Revolution Summit Docuseries ProgramDocument28 pages2023 Food Revolution Summit Docuseries Programelijoja06No ratings yet
- Cardiology 2012 MrcppassDocument127 pagesCardiology 2012 MrcppassRaouf Ra'fat SolimanNo ratings yet
- Acute Coronary SyndromeDocument19 pagesAcute Coronary SyndromeSherree HayesNo ratings yet
- IIA - Altered Tissue PerfusionDocument14 pagesIIA - Altered Tissue PerfusionDharylle CariñoNo ratings yet
- Hartrevalidatie PRL Eng KNGFDocument52 pagesHartrevalidatie PRL Eng KNGFsilkofosNo ratings yet
- Case Reports AbstractsDocument7 pagesCase Reports AbstractsNovie AstiniNo ratings yet
- ECG ErrorsDocument5 pagesECG ErrorsmikeNo ratings yet