You might also like
- Anti ArrhythmicsDocument46 pagesAnti Arrhythmicsmunim1192No ratings yet
- Antidysrhythmic Drugs: Dr. SanoozDocument104 pagesAntidysrhythmic Drugs: Dr. SanoozsanoozarmNo ratings yet
- Cebu Normal University College of NursingDocument7 pagesCebu Normal University College of NursingGwyn RosalesNo ratings yet
- LECT-5B - Patient Case and MISCDocument31 pagesLECT-5B - Patient Case and MISCnonaNo ratings yet
- 69.-AntiarrythmiticsDocument16 pages69.-AntiarrythmiticsireneNo ratings yet
- Anti-Arrhythmic DrugsDocument45 pagesAnti-Arrhythmic Drugssultan khabeebNo ratings yet
- Conduction Defects & ArrythmiasDocument73 pagesConduction Defects & Arrythmiasadamu mohammadNo ratings yet
- Antiarrhythmic Drugs by ZebDocument40 pagesAntiarrhythmic Drugs by ZebFazl UllahNo ratings yet
- Antiarrhythmic DrugsDocument17 pagesAntiarrhythmic DrugsTarek G MustafaNo ratings yet
- Chapter 4 Drugs Used in Arrhythymias(1)Document27 pagesChapter 4 Drugs Used in Arrhythymias(1)Kaye ValenzuelaNo ratings yet
- Antiarrhythmic DrugsDocument116 pagesAntiarrhythmic DrugsJASMEEN RAVALNo ratings yet
- Lecture 8b Obat Anti-AritmiaDocument25 pagesLecture 8b Obat Anti-AritmiaAyu NursantiNo ratings yet
- Summary - Cardio-Oncology-2016-for Web PDFDocument2 pagesSummary - Cardio-Oncology-2016-for Web PDFDya AndryanNo ratings yet
- 3 DrugsforHeartFailureDocument60 pages3 DrugsforHeartFailureJov CelNo ratings yet
- HYPERTENSION Priya FINAL PPT 2Document14 pagesHYPERTENSION Priya FINAL PPT 2Priya Tiwari100% (1)
- Cardiovascular Pharmacology: Antiarrhythmic DrugsDocument80 pagesCardiovascular Pharmacology: Antiarrhythmic DrugsThái Hoà PhạmNo ratings yet
- Cardiac Inotropes in Treatment of Heart Failure Fight (Autosaved)Document32 pagesCardiac Inotropes in Treatment of Heart Failure Fight (Autosaved)Insan IlmanNo ratings yet
- 6 - 2 - CVS Antiarrhythmic 2 by Col AzmatDocument72 pages6 - 2 - CVS Antiarrhythmic 2 by Col AzmatAhmed YTNo ratings yet
- Lecture2 3Document44 pagesLecture2 3Amanda HizerNo ratings yet
- Drugs Acting On CVS-2014Document36 pagesDrugs Acting On CVS-2014كسلان اكتب اسميNo ratings yet
- Updated Lecture July2023-AntiarrthymicsDocument54 pagesUpdated Lecture July2023-Antiarrthymicsg.4ssilaNo ratings yet
- Drugs Used in The Treatment of ArrhythmiasDocument37 pagesDrugs Used in The Treatment of ArrhythmiasChipego ChiyaamaNo ratings yet
- Y2022 - Antihypertensive Agents - Compatibility ModeDocument36 pagesY2022 - Antihypertensive Agents - Compatibility ModeNhân Trần DanhNo ratings yet
- Drug StudyDocument4 pagesDrug StudyCyrene Jasmine CabañesNo ratings yet
- Anti Hypertensive DrugsDocument113 pagesAnti Hypertensive DrugsRobert DowneyNo ratings yet
- Generic Name T Rade Name Lanoxin DigoxinDocument1 pageGeneric Name T Rade Name Lanoxin DigoxinChristopher LeeNo ratings yet
- Diskusi Topik Anestesi GamaDocument65 pagesDiskusi Topik Anestesi Gamakusumagama28No ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- TCA Poisoning SlideDocument66 pagesTCA Poisoning SlideksugamoNo ratings yet
- Case 02 Arrhythmias 2Document23 pagesCase 02 Arrhythmias 2pqp7mpk7v6No ratings yet
- IHD Part 2 - Pharmacology of Angina - RecordedDocument25 pagesIHD Part 2 - Pharmacology of Angina - RecordedSarah SabtiNo ratings yet
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Pheo Presentation FinalDocument52 pagesPheo Presentation FinalArhanNo ratings yet
- Drugs Used in Hypertension: Dr. R. PilvinieneDocument33 pagesDrugs Used in Hypertension: Dr. R. PilvinieneNewteNo ratings yet
- Pharma Cvs Endocrine RespDocument15 pagesPharma Cvs Endocrine RespYuku BabyNo ratings yet
- Antiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIDocument56 pagesAntiaritmia: Frans D. Suyatna Modified by Sulistia 1010 Departemen Farmakologi & Terapeutik FKUIJoshua ObrienNo ratings yet
- Drug Therapy of EpilepsiesDocument43 pagesDrug Therapy of EpilepsiesZobayer Ahmed100% (1)
- Drugs That Affect Cardiovascular SystemDocument35 pagesDrugs That Affect Cardiovascular Systems.khan9211rediffmail.comNo ratings yet
- Vasodil - Ischemic Heart DiseaseDocument52 pagesVasodil - Ischemic Heart DiseaseNorms YoramNo ratings yet
- Obat-Obat NefrotoksikDocument43 pagesObat-Obat Nefrotoksiknursidiq10100% (1)
- HPNDocument32 pagesHPNkaren GoNo ratings yet
- 1. Antiarrhythmics SpmmcDocument40 pages1. Antiarrhythmics SpmmccreativejoburgNo ratings yet
- Journal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesDocument16 pagesJournal Presentation: Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary SyndromesStellaNo ratings yet
- Presentasi Hipertensi BPJS 20518Document109 pagesPresentasi Hipertensi BPJS 20518Dody TamaraNo ratings yet
- Antiarrhythmic DrugsDocument46 pagesAntiarrhythmic DrugsHUZAIFA YAMAANNo ratings yet
- Hydralazine DSDocument2 pagesHydralazine DSAntoniette Jane Martin PathayNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- AdenosineDocument23 pagesAdenosineSabrina ShalhoutNo ratings yet
- Antiarrhythmic AgentsDocument45 pagesAntiarrhythmic AgentsSoh Kae SiangNo ratings yet
- Pharmaceutical chemistry-II: Antihypertensive DrugsDocument5 pagesPharmaceutical chemistry-II: Antihypertensive DrugsMONIKA SINGHNo ratings yet
- Lecture 6 Anti HypertensionDocument40 pagesLecture 6 Anti HypertensionMNGS StudioNo ratings yet
- 1.CVS drugsDocument98 pages1.CVS drugsHarshika KDGNo ratings yet
- Adrenergic DrugsDocument45 pagesAdrenergic DrugsHUZAIFA YAMAANNo ratings yet
- Anti HTNDocument59 pagesAnti HTNzaha shamseerNo ratings yet
- Anti Ar Rythmic S Lecture As Jan 05Document33 pagesAnti Ar Rythmic S Lecture As Jan 05hirschmedNo ratings yet
- Antiarrhythmic DrugsDocument50 pagesAntiarrhythmic DrugsamirNo ratings yet
- gabion-drugstudyCKDDocument5 pagesgabion-drugstudyCKDShiehan Mae ForroNo ratings yet
- L9-Drug Treatment of Epilepsy (BB) - 1Document27 pagesL9-Drug Treatment of Epilepsy (BB) - 1120420314No ratings yet
- Pharmacology for Student and Pupil Nurses and Students in Associated ProfessionsFrom EverandPharmacology for Student and Pupil Nurses and Students in Associated ProfessionsNo ratings yet
- Who 2016 PDFDocument2 pagesWho 2016 PDFRefialy WahyyNo ratings yet
- Cardiovascular Disease EssayDocument9 pagesCardiovascular Disease EssayW.flores07No ratings yet
- Osmosis Is Serious BusinessDocument5 pagesOsmosis Is Serious Businessapi-323720899No ratings yet
- 3 - Focus-Assessed Transthoracic EchocardiographyDocument7 pages3 - Focus-Assessed Transthoracic EchocardiographyMarcelo RibeiroNo ratings yet
- Research Paper For Crec Checking 2Document30 pagesResearch Paper For Crec Checking 2Ella B. CollantesNo ratings yet
- Accident and Emergency (Listening & Role Play) and Caring Elderly (Listening)Document3 pagesAccident and Emergency (Listening & Role Play) and Caring Elderly (Listening)Novianus Ummah SanyNo ratings yet
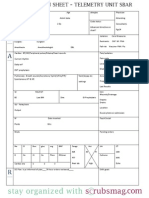
- Nurse Brain Sheet Telemetry Unit SBARDocument1 pageNurse Brain Sheet Telemetry Unit SBARvsosa624No ratings yet
- A Benchmark Study of Machine Learning For Analysis of Signal Feature Extraction Techniques For Blood Pressure Estimation Using Photoplethysmography (PPG)Document17 pagesA Benchmark Study of Machine Learning For Analysis of Signal Feature Extraction Techniques For Blood Pressure Estimation Using Photoplethysmography (PPG)PING KWAN MANNo ratings yet
- PROCEDURE Arterial Pressure Cardiac Output MonitoringDocument7 pagesPROCEDURE Arterial Pressure Cardiac Output MonitoringShreya SinhaNo ratings yet
- Child CPR: Skills Testing ChecklistDocument3 pagesChild CPR: Skills Testing ChecklistTravis TravoltaNo ratings yet
- BplogDocument2 pagesBplogMonir AhamedNo ratings yet
- Medical Surgical Drug StudyDocument45 pagesMedical Surgical Drug StudyMichelle Angela AlombroNo ratings yet
- Product Includes:: Model BP765 Instruction ManualDocument40 pagesProduct Includes:: Model BP765 Instruction ManualMadhuritha RajapakseNo ratings yet
- UTHR LQDA - Appealscourt 24 Jul 23Document23 pagesUTHR LQDA - Appealscourt 24 Jul 23XDL1No ratings yet
- CPR & AED Awareness SurveyDocument38 pagesCPR & AED Awareness Surveydanielkevin19141No ratings yet
- FdarDocument2 pagesFdarkasandra dawn Beriso67% (3)
- PNM 2018 358-360 PDFDocument3 pagesPNM 2018 358-360 PDFputriNo ratings yet
- Echocardiography Assessment of Coronary Artery DiseaseDocument28 pagesEchocardiography Assessment of Coronary Artery DiseaseYibeltal AssefaNo ratings yet
- Pagewriter Xli Users GuideDocument129 pagesPagewriter Xli Users Guidemebme2022No ratings yet
- Clinical Guide for Safe AnticoagulationDocument9 pagesClinical Guide for Safe AnticoagulationMhmad MayhobNo ratings yet
- Respiratory Case Study 6 PDFDocument2 pagesRespiratory Case Study 6 PDFZainab HakeemNo ratings yet
- A Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and MidwiferyDocument13 pagesA Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and Midwiferyhsiria100% (2)
- Quiz: Obstetrics fetal developmentDocument1 pageQuiz: Obstetrics fetal developmentDENNIS N. MUÑOZNo ratings yet
- Lecture 2-Cardiovascular AssessmentDocument28 pagesLecture 2-Cardiovascular AssessmentSamuel Sebastian SirapanjiNo ratings yet
- Pulmonary Embolism: Ahmad Faeez Aleeffuddin Bin Mohamad Bidin Mentor:Encik SamsuddinDocument22 pagesPulmonary Embolism: Ahmad Faeez Aleeffuddin Bin Mohamad Bidin Mentor:Encik SamsuddinJuni Zuhairah Abd GhafarNo ratings yet
- Virani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdateDocument490 pagesVirani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdatehendridunantikoNo ratings yet
- 6662 - ARB - Nurlia Rizky Andri S - 21904101038 - Reza Rahma Tazkia - 21904101039Document4 pages6662 - ARB - Nurlia Rizky Andri S - 21904101038 - Reza Rahma Tazkia - 21904101039Reza Rahma TazkiaNo ratings yet
- Note Making 8 Marks PDFDocument5 pagesNote Making 8 Marks PDFRishiraj VermaNo ratings yet
- Cardiac UltrasoundDocument72 pagesCardiac Ultrasoundramon100% (6)
- Exercises On The Cardiovascular SystemDocument2 pagesExercises On The Cardiovascular SystemNguyễn Thị Hương Y.K53HNo ratings yet