You might also like
- Test Bank For Clayton's Basic Pharmacology For Nurses 18th Edition by Willihnganz All ChaptersDocument350 pagesTest Bank For Clayton's Basic Pharmacology For Nurses 18th Edition by Willihnganz All Chaptersabbie100% (3)
- Pharmacists Council of Nigeria PCN Past Questions PDF DownloadDocument6 pagesPharmacists Council of Nigeria PCN Past Questions PDF DownloadCharles Obaleagbon80% (5)
- BaddiDocument22 pagesBaddiraj.kajaniya60% (5)
- Sedation of Patients in ICUDocument9 pagesSedation of Patients in ICUAlfrin AntonyNo ratings yet
- Brain Resuscitation and Protection MutiaraDocument30 pagesBrain Resuscitation and Protection MutiaraMutiaraNo ratings yet
- 05 IV Induction Agents PDFDocument0 pages05 IV Induction Agents PDFjuniorebinda100% (1)
- IV Induction Agents UMAIDDocument63 pagesIV Induction Agents UMAIDUmaid Mirza100% (1)
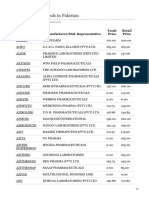
- Azithromycin Brands in Pakistan PDFDocument4 pagesAzithromycin Brands in Pakistan PDFibNo ratings yet
- Swot Analysis of Medco Health SolutionDocument5 pagesSwot Analysis of Medco Health SolutionAbdul Qayoom100% (1)
- Benzodiazepines: Ben Tsutaoka, PharmdDocument6 pagesBenzodiazepines: Ben Tsutaoka, Pharmdrefimaya arlitaNo ratings yet
- Research ProjectDocument9 pagesResearch ProjectMohamed EssamNo ratings yet
- Intravenous AnestheticsDocument5 pagesIntravenous AnestheticsPM Basiloy - AloNo ratings yet
- Lecture On Pharmacology of Anesthetic Drugs: Yizez Mebratu 23APR11Document90 pagesLecture On Pharmacology of Anesthetic Drugs: Yizez Mebratu 23APR11Tefera LeteboNo ratings yet
- Uia 13 DELAYED AWAKENING OR EMERGENCE FROM ANAESTHESIADocument3 pagesUia 13 DELAYED AWAKENING OR EMERGENCE FROM ANAESTHESIAsunny kumarNo ratings yet
- General Anesthetics AbeerDocument45 pagesGeneral Anesthetics AbeerYousef JafarNo ratings yet
- Cology Lab AssignmntDocument4 pagesCology Lab Assignmntamama khanNo ratings yet
- Desirable Properties of PSA Pharmacologic AgentsDocument42 pagesDesirable Properties of PSA Pharmacologic AgentsMarjan HusniNo ratings yet
- Medications For Analgesia and Sedation in The Intensive Care Unit: An OverviewDocument5 pagesMedications For Analgesia and Sedation in The Intensive Care Unit: An OverviewJohn MaynhamNo ratings yet
- Medicamentos Sedacion UCI PDFDocument5 pagesMedicamentos Sedacion UCI PDFAnnison Hector Ramos BravoNo ratings yet
- Fentanyl Citrate Injection, USP: RX Only DescriptionDocument7 pagesFentanyl Citrate Injection, USP: RX Only DescriptionWidy WidyNo ratings yet
- Pharmacology of AnaestheticDocument72 pagesPharmacology of AnaestheticOmar HamwiNo ratings yet
- Delayed Awakening From AnaesthesiaDocument3 pagesDelayed Awakening From AnaesthesiaSenthooran ArudshivsmNo ratings yet
- Module 4Document18 pagesModule 4nishanth nishanthNo ratings yet
- Pharmacodynamics (Agonists: Mechanisms of Drug Actions)Document36 pagesPharmacodynamics (Agonists: Mechanisms of Drug Actions)Wajid HusseinNo ratings yet
- Antiepileptic DrugsDocument65 pagesAntiepileptic DrugsZarish IftikharNo ratings yet
- 08 .麻醉用藥 - 邱全秀Document62 pages08 .麻醉用藥 - 邱全秀kenny631653No ratings yet
- BenzodiazepinesDocument6 pagesBenzodiazepinesRoman MamunNo ratings yet
- AntiepilepticsDocument13 pagesAntiepilepticstbuyinza21apNo ratings yet
- Pharmacology of AntiepilepticDocument36 pagesPharmacology of AntiepilepticManWol JangNo ratings yet
- Pharmacotherapy of Bronchial AsthmaDocument7 pagesPharmacotherapy of Bronchial AsthmaAhmedshaker21100% (2)
- Evaluation and Management of Delayed Awakening or Emergence From AnaesthesiaDocument19 pagesEvaluation and Management of Delayed Awakening or Emergence From AnaesthesiaMuhammad UmairNo ratings yet
- LI Case 2 (Pharmacological Properties of Propanolol)Document2 pagesLI Case 2 (Pharmacological Properties of Propanolol)adtyadaviaNo ratings yet
- Autonomic Nervous System-2Document8 pagesAutonomic Nervous System-2محمد علي حميدNo ratings yet
- IV Anesthetic AgentsDocument72 pagesIV Anesthetic AgentsRaghavendra PrasadNo ratings yet
- Presentation 2Document20 pagesPresentation 2Muhammad UmairNo ratings yet
- ART Rugs and Nfusions: A. PolicyDocument7 pagesART Rugs and Nfusions: A. PolicyZoelNo ratings yet
- AaasDocument109 pagesAaaswaqar44No ratings yet
- Pharmacology Give Reasons (NHCON Calicut)Document7 pagesPharmacology Give Reasons (NHCON Calicut)Ameesha JojoNo ratings yet
- Cardiovascular Pharmacology PDFDocument20 pagesCardiovascular Pharmacology PDFMelanie PrinceNo ratings yet
- Psychoactive DrugsDocument24 pagesPsychoactive DrugsIshaani GargNo ratings yet
- Lect 19 General AnesthesiaDocument7 pagesLect 19 General AnesthesiaBrandon AviciiNo ratings yet
- Central Nervous System DepressantsDocument11 pagesCentral Nervous System Depressantsاسامه عمر عثمانNo ratings yet
- Anestesi Intravena: A. KetamineDocument2 pagesAnestesi Intravena: A. KetamineFatinahNo ratings yet
- AnaestheticsDocument25 pagesAnaestheticsmadeha goharNo ratings yet
- Mekanisme Local AnastesiDocument10 pagesMekanisme Local AnastesiAndrean HeryantoNo ratings yet
- TIVA - Copy (2) - Copy-1Document34 pagesTIVA - Copy (2) - Copy-1Keerthikumar Parvatha100% (2)
- General AnestheticsDocument34 pagesGeneral AnestheticsHemanathan Praem100% (1)
- Halcion Triazolam Tablets, USP CIV: DescriptionDocument14 pagesHalcion Triazolam Tablets, USP CIV: DescriptionAlberto JaramilloNo ratings yet
- Preoperative Patient AssessmentDocument5 pagesPreoperative Patient Assessmenthonovezaann.a.campita.ctucvmNo ratings yet
- General AnaestheticsDocument39 pagesGeneral AnaestheticsMBBS AspirantNo ratings yet
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
- RANASINGHE Basic Pharmacology and IV HypnoticsDocument34 pagesRANASINGHE Basic Pharmacology and IV HypnoticsDagimNo ratings yet
- Delayed Recovery After AnaesthesiaDocument5 pagesDelayed Recovery After Anaesthesiakoolstarone100% (1)
- 2016 Pharmacology of Sedative-HypnoticDocument46 pages2016 Pharmacology of Sedative-HypnoticFansisca SiallaganNo ratings yet
- Journal Course Evidence Based Use of Nonopioid Analgesics August 2018Document7 pagesJournal Course Evidence Based Use of Nonopioid Analgesics August 2018DesywinNo ratings yet
- Anti Epileptic AgentsDocument64 pagesAnti Epileptic AgentsPrincess VanquirayNo ratings yet
- Michael Jackson's Cause of DeathDocument40 pagesMichael Jackson's Cause of DeathYeni SuwitaNo ratings yet
- Adrenergic AntagonistsDocument23 pagesAdrenergic AntagonistsMirza Shaharyar BaigNo ratings yet
- Drug InteractionsDocument21 pagesDrug InteractionsPawan Deshmukh100% (1)
- Premedication and Other Prophylactic MeasuresDocument39 pagesPremedication and Other Prophylactic Measuresanugerah_buang3842No ratings yet
- Pharmacology NMB Ds and Anti Cholinesterase S FinalDocument8 pagesPharmacology NMB Ds and Anti Cholinesterase S FinalPamella Kusuma WerdanieNo ratings yet
- Overdose in A Patient With Parkinson Disease - 231116 - 122758Document5 pagesOverdose in A Patient With Parkinson Disease - 231116 - 122758joonabil29No ratings yet
- Barbiturate ToxicityDocument12 pagesBarbiturate ToxicityDayagNo ratings yet
- An Introduction to Mechanisms in Pharmacology and TherapeuticsFrom EverandAn Introduction to Mechanisms in Pharmacology and TherapeuticsNo ratings yet
- BCS Classification of Some Drugs:: S/No Medicine Strength Solubility Permeability ClassDocument6 pagesBCS Classification of Some Drugs:: S/No Medicine Strength Solubility Permeability Classmuhammad shoaibNo ratings yet
- Abas MedicateDocument20 pagesAbas MedicateRather IrfanNo ratings yet
- Module 10 Rotation Schedule OriginalDocument5 pagesModule 10 Rotation Schedule Originalapi-372924050No ratings yet
- Chinse Pharmacopoeia 2015 - Vol. 1Document2,262 pagesChinse Pharmacopoeia 2015 - Vol. 1dennis abarca calderónNo ratings yet
- Avil 201703Document2 pagesAvil 201703Nirajit Krishna 8A J640No ratings yet
- Pharmabites 9 10 07Document1 pagePharmabites 9 10 07api-3707097No ratings yet
- Extemporaneous Review PDFDocument52 pagesExtemporaneous Review PDFKomang Prawira Nata NugrahaNo ratings yet
- Guidelines For The Advertisement of Drugs, Herbal Medicines, Cosmetics, Medical Devices & Household ChemicalsDocument8 pagesGuidelines For The Advertisement of Drugs, Herbal Medicines, Cosmetics, Medical Devices & Household ChemicalssboaduappiahNo ratings yet
- Public Health: DevelopingDocument3 pagesPublic Health: DevelopingfelminaNo ratings yet
- Pivot 4a Lesson Exemplar in Mapeh 6Document7 pagesPivot 4a Lesson Exemplar in Mapeh 6Crisente BarcelonNo ratings yet
- Bioequivalence of Oxcarbazepine Oral Suspension vs. Film-Coated Tablet in Healthy Chinese Male SubjectsDocument8 pagesBioequivalence of Oxcarbazepine Oral Suspension vs. Film-Coated Tablet in Healthy Chinese Male SubjectsdarismendyNo ratings yet
- Industrial Training at Benham Pharmaceutical LTDDocument37 pagesIndustrial Training at Benham Pharmaceutical LTDRabbiiKhanNo ratings yet
- Official: Á641Ñ Completeness of SolutionDocument1 pageOfficial: Á641Ñ Completeness of SolutionDilawar BakhtNo ratings yet
- Appendix 2A - Application Checklist - ICH - NDA - GDADocument39 pagesAppendix 2A - Application Checklist - ICH - NDA - GDAnasimNo ratings yet
- DesloratadineDocument6 pagesDesloratadineEliza TelamianaNo ratings yet
- Silver Book Part A Medication Management ID3104Document7 pagesSilver Book Part A Medication Management ID3104Anton BalansagNo ratings yet
- Pharmacy ManagementDocument10 pagesPharmacy ManagementLâm Tường NguyễnNo ratings yet
- Brilinta RXDocument10 pagesBrilinta RXravi_bhateja_2No ratings yet
- Patient Medication Profile ActivityDocument1 pagePatient Medication Profile ActivityxylentknightNo ratings yet
- Jessica Alxan: EducationDocument3 pagesJessica Alxan: Educationapi-526214071No ratings yet
- Pharmasist LoksewaDocument5 pagesPharmasist LoksewaAashish BhattaraiNo ratings yet
- Quiz Lecture 2Document4 pagesQuiz Lecture 2Hoang Uyen Vy NguyenNo ratings yet
- Layout of Pharmacy in HospitalDocument8 pagesLayout of Pharmacy in HospitalUmar JadoonNo ratings yet
- A Survey Exploring The Knowledge and Perceptions of Senior Medical Students in Nepal Toward Generic MedicinesDocument6 pagesA Survey Exploring The Knowledge and Perceptions of Senior Medical Students in Nepal Toward Generic MedicinesDavids MarinNo ratings yet
- DS SangobionDocument1 pageDS SangobionLarr SumalpongNo ratings yet