You might also like
- Healers Versus Stealers: How to Outsmart the Thief in Your Dental PracticeFrom EverandHealers Versus Stealers: How to Outsmart the Thief in Your Dental PracticeNo ratings yet
- Classification of Extraction Sockets - Dennis TarnowDocument1 pageClassification of Extraction Sockets - Dennis TarnowManan AroraNo ratings yet
- 1.taper of Clinical Preparations For Cast RestorationsDocument8 pages1.taper of Clinical Preparations For Cast RestorationsAle Zuza100% (1)
- Introduction of A Novel Anatomic Recession RatioDocument11 pagesIntroduction of A Novel Anatomic Recession Ratiojuanita enriquezNo ratings yet
- Clinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic ReviewDocument13 pagesClinical Outcomes of Vertical Bone Augmentation To Enable Dental Implant Placement: A Systematic Reviewvanessa_werbickyNo ratings yet
- Drill Less Air AbrasionDocument4 pagesDrill Less Air AbrasionMaria IvanaNo ratings yet
- Influence of Restoration Thickness and Dental Bonding Surface On The Fracture Resistance of Full-Coverage Occlusal Veneers Made From Lithium Disilicate CeramicDocument9 pagesInfluence of Restoration Thickness and Dental Bonding Surface On The Fracture Resistance of Full-Coverage Occlusal Veneers Made From Lithium Disilicate CeramicKennya GarnicaNo ratings yet
- Ferrule Comes FirstDocument8 pagesFerrule Comes FirstAndras KuthiNo ratings yet
- New Multi-Layered Zirconias: Composition, Microstructure and TranslucencyDocument10 pagesNew Multi-Layered Zirconias: Composition, Microstructure and TranslucencyChristianNo ratings yet
- Semilunar Coronally Repositioned FlapDocument5 pagesSemilunar Coronally Repositioned FlapTarun Kumar Bhatnagar100% (1)
- Ada CodesDocument4 pagesAda CodestedyNo ratings yet
- Atlas of Removable Orthodontic Appliances PDFDocument151 pagesAtlas of Removable Orthodontic Appliances PDFStephanie Perkins75% (4)
- MDN Femoral Retrograde Intramedullary Fixation Surgical Technique 97-2252-009-01 Rev2 09 2011 PDFDocument22 pagesMDN Femoral Retrograde Intramedullary Fixation Surgical Technique 97-2252-009-01 Rev2 09 2011 PDFcuki5No ratings yet
- WCET NNG ETN Book 2020 PDFDocument179 pagesWCET NNG ETN Book 2020 PDFaryNo ratings yet
- Post Anesthesia Care (PACU) GuidelinesDocument9 pagesPost Anesthesia Care (PACU) GuidelinesRaluca LNo ratings yet
- Race 2018 Final For DR PDFDocument427 pagesRace 2018 Final For DR PDFKarthi KeyanNo ratings yet
- Smile Analysis What To MeasureDocument6 pagesSmile Analysis What To MeasureAli RazaNo ratings yet
- Expansion of The Zone of Keratinised Tissue For Healthy Implant Abutment Interface Using Deepithelized Amnion:Chorion AllograftDocument6 pagesExpansion of The Zone of Keratinised Tissue For Healthy Implant Abutment Interface Using Deepithelized Amnion:Chorion AllograftzethyhanumNo ratings yet
- Qi 52 2 Sampaio p104Document7 pagesQi 52 2 Sampaio p104jcNo ratings yet
- Cite Share Labial Strip Gingival Graft For The Reconstruction of Severely Distorted Mucogingival Defects - Urban 2020Document9 pagesCite Share Labial Strip Gingival Graft For The Reconstruction of Severely Distorted Mucogingival Defects - Urban 2020Claudio GuzmanNo ratings yet
- Tunneled Coronally Advanced Flap For The Treatment of Isolated Gingival Recessions With Deficient PapillaDocument14 pagesTunneled Coronally Advanced Flap For The Treatment of Isolated Gingival Recessions With Deficient Papillafloressam2000No ratings yet
- Rotation Reciprocation or CombinationDocument30 pagesRotation Reciprocation or CombinationvanillalavenderNo ratings yet
- Tuberosidad HistologiaDocument10 pagesTuberosidad HistologiaMaximiliano Jara ContrerasNo ratings yet
- J Esthet Restor Dent - 2023 - Sulaiman - Zirconia Restoration Types Properties Tooth Preparation Design and Bonding ADocument7 pagesJ Esthet Restor Dent - 2023 - Sulaiman - Zirconia Restoration Types Properties Tooth Preparation Design and Bonding AAlfred OrozcoNo ratings yet
- The Inverse Injection Layering TechniqueDocument16 pagesThe Inverse Injection Layering TechniqueJuan Francisco CamposNo ratings yet
- Guia Anterior - Gonzalez Hernandez-61-2Document12 pagesGuia Anterior - Gonzalez Hernandez-61-2Fred TorresNo ratings yet
- Crown Lenghtening - Gummy Smile PDFDocument13 pagesCrown Lenghtening - Gummy Smile PDFVladislava GanevaNo ratings yet
- Jdo Vol 64 UpdatedDocument85 pagesJdo Vol 64 UpdatedKanchit SuwanswadNo ratings yet
- The Simultaneous Modeling Technique Closing Gaps in PosteriorsDocument24 pagesThe Simultaneous Modeling Technique Closing Gaps in PosteriorsÄpriolia SuNo ratings yet
- Hero Shaper Final 9Document2 pagesHero Shaper Final 9shamshuddin patelNo ratings yet
- Spear-Approaches To Vertical DimensionDocument11 pagesSpear-Approaches To Vertical DimensionMario Zúñiga Gonzales100% (2)
- Anderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinDocument4 pagesAnderson (1985) A Comparison of Digital and Optical Criteria For Detecting Carious DentinОлександр БайдоNo ratings yet
- Injectabletechniquefordirectprovisionalrestoration PDFDocument5 pagesInjectabletechniquefordirectprovisionalrestoration PDFCSilva16No ratings yet
- 1 s2.0 S1073874621000451 MainDocument4 pages1 s2.0 S1073874621000451 MainMarcos Gómez SosaNo ratings yet
- Biologically Oriented Preparation Technique For SurgicallyDocument6 pagesBiologically Oriented Preparation Technique For SurgicallyAbdelrahman Galal100% (1)
- Comparison of Failure and Complication Risks of Porcelain Laminate and Indirect Resin Veneer Restoration A Meta-Analysis PDFDocument8 pagesComparison of Failure and Complication Risks of Porcelain Laminate and Indirect Resin Veneer Restoration A Meta-Analysis PDFLinda Garcia PNo ratings yet
- Matias AnghileriDocument32 pagesMatias AnghileriSilvia Fernanda Rosa100% (1)
- A Novel B-Titanium Alloy Orthodontic Wire: SciencedirectDocument5 pagesA Novel B-Titanium Alloy Orthodontic Wire: Sciencedirectsolodont1No ratings yet
- Adams ClaspDocument16 pagesAdams ClaspNimrah Razzaque MemonNo ratings yet
- XxxDenture Soft Lining Materials Clinical IndicationsDocument5 pagesXxxDenture Soft Lining Materials Clinical IndicationsrekabiNo ratings yet
- 10 1016@j Prosdent 2020 05 007Document5 pages10 1016@j Prosdent 2020 05 007Anjali DuttaNo ratings yet
- The Radix Entomolaris and Paramolaris: Clinical Approach in EndodonticsDocument6 pagesThe Radix Entomolaris and Paramolaris: Clinical Approach in EndodonticsPankajkumar GuptaNo ratings yet
- Art Perfil de Emergencia Implantes PDFDocument7 pagesArt Perfil de Emergencia Implantes PDFdiego alenadro trujilloNo ratings yet
- PRD 22 5 Magne1Document10 pagesPRD 22 5 Magne1sofa83No ratings yet
- 04-05-2012 Review On Radix Entomolaris and ParamolarisDocument23 pages04-05-2012 Review On Radix Entomolaris and ParamolarisjyotsnasistlaNo ratings yet
- Extract Manauta Layers2Document33 pagesExtract Manauta Layers2Sociedad Dentotal AraucaníaNo ratings yet
- Orthodontic Update - April 2020 PDFDocument54 pagesOrthodontic Update - April 2020 PDFMaria TzagarakiNo ratings yet
- An Overview of The Surgical Correction of Dentofacial DeformityDocument9 pagesAn Overview of The Surgical Correction of Dentofacial DeformityAhmad AssariNo ratings yet
- Traumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental AcademyDocument43 pagesTraumatic Injuries of The Tooth / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- 2019 Tucker Syllabus 2afee7be57Document103 pages2019 Tucker Syllabus 2afee7be57Landon AllenNo ratings yet
- NewtonDocument63 pagesNewtondentisdoc100% (2)
- Prevalence of Radix Entamolaris in Kashmiri PopulationDocument7 pagesPrevalence of Radix Entamolaris in Kashmiri Populationarshad khandayNo ratings yet
- Surgically-Assisted Rapid Palatal Expansion For Management of Transverse Maxillary DeficiencyDocument3 pagesSurgically-Assisted Rapid Palatal Expansion For Management of Transverse Maxillary DeficiencyDaniela CastilloNo ratings yet
- 18 1994 - John Preston - The Golden Proportion RevistedDocument5 pages18 1994 - John Preston - The Golden Proportion RevistedSilvia KriNo ratings yet
- Papper PeriodDocument12 pagesPapper PeriodLoretoReyesMoralesNo ratings yet
- Plonk A 2018Document8 pagesPlonk A 2018Jazmín TortellaNo ratings yet
- Third Molars: A Dilemma! or Is It?: Clinicians' CornerDocument6 pagesThird Molars: A Dilemma! or Is It?: Clinicians' CornerElizabeth CortésNo ratings yet
- Orthodontics For Undersized Teeth: The Bioclear MethodDocument7 pagesOrthodontics For Undersized Teeth: The Bioclear MethodThe Bioclear ClinicNo ratings yet
- Article CL III MalocclusionDocument6 pagesArticle CL III MalocclusionAbhijeet KaduNo ratings yet
- Exo OrthoDocument8 pagesExo OrthoEndriyana NovitasariNo ratings yet
- Ortho Organizers Catalog 2010-2011Document291 pagesOrtho Organizers Catalog 2010-2011Gloria Diana Aguilar PizzurnoNo ratings yet
- Orthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerFrom EverandOrthodontic Biomechanics: Treatment Of Complex Cases Using Clear AlignerNo ratings yet
- Intrusion With Mini ImplantDocument13 pagesIntrusion With Mini Implantdrzana78100% (1)
- Oncology-Study of Cancer Cellular AbberationDocument43 pagesOncology-Study of Cancer Cellular AbberationIrwan M. IskoberNo ratings yet
- B.D.S Course Regulations/Syllabus: (With Effect From 2010-11 Onwards)Document127 pagesB.D.S Course Regulations/Syllabus: (With Effect From 2010-11 Onwards)rkNo ratings yet
- Assessment Nursing Diagnosis Rationale Planning Nursing Action Rationale EvaluationDocument2 pagesAssessment Nursing Diagnosis Rationale Planning Nursing Action Rationale EvaluationJames Czar FontanillaNo ratings yet
- Demo DexDocument4 pagesDemo DexIrina CornilovNo ratings yet
- Low Back Pain Case Study - A Nasty One! But A Good Outcome. - Witty, Pask & BuckinghamDocument4 pagesLow Back Pain Case Study - A Nasty One! But A Good Outcome. - Witty, Pask & BuckinghamermanmahendraNo ratings yet
- Drug Name Mechanism of Action Indication Contraindication Advers Effects Nursing Responsibilities Generic Name: SkinDocument1 pageDrug Name Mechanism of Action Indication Contraindication Advers Effects Nursing Responsibilities Generic Name: SkinsalwaNo ratings yet
- 1 Exercise ERD 1Document2 pages1 Exercise ERD 1Yashil Yudhisthir BhurtunNo ratings yet
- Benign Febrile SeizureDocument15 pagesBenign Febrile SeizureRhaffy Bearneza RapaconNo ratings yet
- 9.b. Revision of Annex A Medical and Eyesight Standards From MSN 1839Document33 pages9.b. Revision of Annex A Medical and Eyesight Standards From MSN 1839Vijay BhaskarNo ratings yet
- Surgery Syllabus 2010.12Document7 pagesSurgery Syllabus 2010.12AsterzebuleNo ratings yet
- Hand Burns: Karen J. Kowalske, MD, David G. Greenhalgh, MD, Scott R. Ward, PHD, PTDocument4 pagesHand Burns: Karen J. Kowalske, MD, David G. Greenhalgh, MD, Scott R. Ward, PHD, PTalizzxNo ratings yet
- Atherosclerosis & Trombosis Dr. FaturochmanDocument50 pagesAtherosclerosis & Trombosis Dr. FaturochmanPutry RizqiaNo ratings yet
- Spinal Cord InjuriesDocument49 pagesSpinal Cord Injuriesjustin_saneNo ratings yet
- Hysterical PsychosisDocument13 pagesHysterical PsychosisAllan DiasNo ratings yet
- A Case Report On Multifetal PregnancyDocument5 pagesA Case Report On Multifetal PregnancyThreecee VelezNo ratings yet
- Reynaud's DseDocument6 pagesReynaud's DseKengkai MiiNo ratings yet
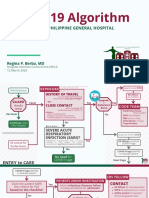
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Pharm Drugs MasterDocument42 pagesPharm Drugs MasterJessica Esper EmbresciaNo ratings yet
- Statutory Construction 1st Sem Finals Review 2019Document10 pagesStatutory Construction 1st Sem Finals Review 2019MiltoniusKNo ratings yet
- Pregabalin An Anticonvulsant DrugDocument2 pagesPregabalin An Anticonvulsant DrugmeimeiliuNo ratings yet
- Type 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsDocument6 pagesType 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsTrifosa Ika Septiana EryaniNo ratings yet
- Case Study: Renal Disease in Type 1 Diabetes: PresentationDocument1 pageCase Study: Renal Disease in Type 1 Diabetes: PresentationadawiahxxNo ratings yet
- Running Head: Current Bio-Terrorism Issues 1Document6 pagesRunning Head: Current Bio-Terrorism Issues 1api-400900026No ratings yet
- Esthetics in Dental ImplantsDocument87 pagesEsthetics in Dental ImplantsRavi Uttara100% (3)
- Just Another Sebaceous Cyst?: I. Clinical QuestionDocument3 pagesJust Another Sebaceous Cyst?: I. Clinical QuestionJaessa FelicianoNo ratings yet
- Examples of Level 6 WritingDocument3 pagesExamples of Level 6 WritingBlossomsky96No ratings yet