You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- MNT Case Study 1 Spring 2017Document35 pagesMNT Case Study 1 Spring 2017api-332216940No ratings yet
- Final Disorders of Perception ShubhiDocument56 pagesFinal Disorders of Perception ShubhiShubhiAggarwal100% (1)
- Hematologi ModulDocument67 pagesHematologi ModulSyifa Mahmud Syukran Akbar100% (1)
- Nucleic Acids As Genetic Information CarriersDocument32 pagesNucleic Acids As Genetic Information Carriersstevensb055100% (4)
- Reviewer Fundamentals of NursingDocument22 pagesReviewer Fundamentals of NursingDarren Flores100% (1)
- Haimovicis Vascular SurgeryDocument1,219 pagesHaimovicis Vascular SurgeryaquijadaNo ratings yet
- 8 - Blood Banking and SerologyDocument4 pages8 - Blood Banking and SerologyRanndolf Javier80% (5)
- Neoplasia QuizDocument9 pagesNeoplasia QuizDocAxi Maximo Jr Axibal67% (6)
- Pathophysiology of Atherosclerosis, Thrombosis and EmbolismDocument4 pagesPathophysiology of Atherosclerosis, Thrombosis and EmbolismKeshant Samaroo100% (1)
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesDocument23 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and Rationalesalexis_borj100% (1)
- Teachers Mannual English Full MarksDocument84 pagesTeachers Mannual English Full Marksgo67% (3)
- Promoting Healthy NutritionDocument26 pagesPromoting Healthy NutritionJose Fernando Díez Concha100% (1)
- Solar Return ReportDocument5 pagesSolar Return ReportJOYYANo ratings yet
- E RDocument10 pagesE Rroy_linaoNo ratings yet
- Annual Report of Durdans HospitalDocument176 pagesAnnual Report of Durdans HospitaloshanNo ratings yet
- ScreenshotDocument1 pageScreenshotSyifa Mahmud Syukran AkbarNo ratings yet
- Lampiran - Moderators of Treatment Efficacy in Individualized Metacognitive Training Metacognitive Training For Psychosis (MCT-) 2020Document8 pagesLampiran - Moderators of Treatment Efficacy in Individualized Metacognitive Training Metacognitive Training For Psychosis (MCT-) 2020Syifa Mahmud Syukran AkbarNo ratings yet
- HF DeaDocument53 pagesHF DeaSyifa Mahmud Syukran AkbarNo ratings yet
- Heart Failure: Yos Akbar IrmansyahDocument49 pagesHeart Failure: Yos Akbar IrmansyahSyifa Mahmud Syukran AkbarNo ratings yet
- Heart Failure & CardiometabolicDocument99 pagesHeart Failure & CardiometabolicSyifa Mahmud Syukran AkbarNo ratings yet
- Dębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuDocument12 pagesDębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuSyifa Mahmud Syukran AkbarNo ratings yet
- AFib GuidlinesDocument4 pagesAFib GuidlinesSyifa Mahmud Syukran AkbarNo ratings yet
- Cardiovascular Physical Examination - SyifaDocument66 pagesCardiovascular Physical Examination - SyifaSyifa Mahmud Syukran AkbarNo ratings yet
- Case Study Amanda Loscerbo Atrial FibrilationDocument6 pagesCase Study Amanda Loscerbo Atrial FibrilationSyifa Mahmud Syukran AkbarNo ratings yet
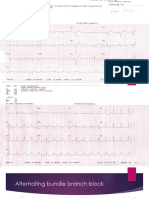
- Alternating Bundle Branch BlockDocument9 pagesAlternating Bundle Branch BlockSyifa Mahmud Syukran AkbarNo ratings yet
- Dilation and CurettageDocument8 pagesDilation and CurettageIrish Eunice FelixNo ratings yet
- Neonatal Respiratory Distress SyndromenhschoicesDocument6 pagesNeonatal Respiratory Distress SyndromenhschoicessehatkanNo ratings yet
- Research Paper - Drug Addiction and AbusDocument5 pagesResearch Paper - Drug Addiction and AbusAvel BadilloNo ratings yet
- 1, Internship Report Tayyba 7th 2020.-1Document21 pages1, Internship Report Tayyba 7th 2020.-1S M Abrar HassanNo ratings yet
- Document 29Document9 pagesDocument 29Mohammad Sabihul HaqueNo ratings yet
- 1 - Introduction of PathologyDocument19 pages1 - Introduction of PathologyseifosmanNo ratings yet
- ACDS Patch Testing To Propylene Glycol2.7.18Document20 pagesACDS Patch Testing To Propylene Glycol2.7.18Henry NguyenNo ratings yet
- KP Burning Mouth SyndromeDocument23 pagesKP Burning Mouth SyndromemuhammadNo ratings yet
- 2018 - RCOST - Scientific ProgramDocument17 pages2018 - RCOST - Scientific ProgramGym NoppadonNo ratings yet
- Streptococcus PyogenesDocument11 pagesStreptococcus PyogenesJimson Marc DuranNo ratings yet
- Wolf PresentationDocument35 pagesWolf PresentationTahir Bin AbdullahNo ratings yet
- Raised Erythrocyte Sedimentation Rate Signals HearDocument6 pagesRaised Erythrocyte Sedimentation Rate Signals HearKeith Mark AlmarinesNo ratings yet
- Genius Case StudyDocument10 pagesGenius Case StudychengadNo ratings yet
- Capstone IdeasDocument9 pagesCapstone IdeastijunkNo ratings yet
- Freezing in ParkinsonDocument14 pagesFreezing in ParkinsonGermaine Sperberg DuhartNo ratings yet
- Psychoanalytically InformedDocument15 pagesPsychoanalytically InformedNéstor X. PortalatínNo ratings yet