You might also like
- Application 2011 2012Document12 pagesApplication 2011 2012dbreynaeNo ratings yet
- Handbook: 2499 Main Street Klamath Falls, OR 97601 541-882-4151 Welcome!Document14 pagesHandbook: 2499 Main Street Klamath Falls, OR 97601 541-882-4151 Welcome!api-326416336No ratings yet
- Preschool Parent Handbook August 2016Document11 pagesPreschool Parent Handbook August 2016api-246217621No ratings yet
- Elementary Disclosure Document Sharley Bradley ELP First Grade 2019-2020 Hawthorne Elementary, Room 6Document6 pagesElementary Disclosure Document Sharley Bradley ELP First Grade 2019-2020 Hawthorne Elementary, Room 6api-234404321No ratings yet
- EHMS HandbookDocument7 pagesEHMS HandbookjoezanottoNo ratings yet
- LeConte Newsletter Oct 2011Document7 pagesLeConte Newsletter Oct 2011pazchannelsNo ratings yet
- Newsletter 9 14Document3 pagesNewsletter 9 14api-310256368No ratings yet
- Atoka Elementary School's 5 Grade Classroom Rules, Policies, & Procedures 2016-2017Document5 pagesAtoka Elementary School's 5 Grade Classroom Rules, Policies, & Procedures 2016-2017api-351301719No ratings yet
- Curriculum Night: 4th GradeDocument19 pagesCurriculum Night: 4th Gradeapi-294074853No ratings yet
- Afnorth Elementary Handbook - 2015-2016Document21 pagesAfnorth Elementary Handbook - 2015-2016api-194582413No ratings yet
- REC Newsletter February 2016Document12 pagesREC Newsletter February 2016Reynella East CollegeNo ratings yet
- Student-Parent Handbook 2023-24Document22 pagesStudent-Parent Handbook 2023-24api-292325707No ratings yet
- Welcome To Mrs. Kirk's Fifth Grade Class!: Teaching PhilosophyDocument5 pagesWelcome To Mrs. Kirk's Fifth Grade Class!: Teaching Philosophyapi-287198374No ratings yet
- GEMS SCHOOL - Parent HandbookDocument33 pagesGEMS SCHOOL - Parent HandbookMoaz Mohd Al-ShiekhNo ratings yet
- EHMS Handbook English 15-16Document7 pagesEHMS Handbook English 15-16teacherdarNo ratings yet
- Heaton Avenue Ofsted Report 2008Document12 pagesHeaton Avenue Ofsted Report 2008eikratsNo ratings yet
- Sept 9 Newsletter 2012Document6 pagesSept 9 Newsletter 2012api-108443703No ratings yet
- 01 Info Brochure 2013-14Document11 pages01 Info Brochure 2013-14api-234678525No ratings yet
- School Happenings: 13726 N.State Road 245 Lamar, IN 47550Document7 pagesSchool Happenings: 13726 N.State Road 245 Lamar, IN 47550api-217089716No ratings yet
- Oct. 2011 Gator GazetteDocument6 pagesOct. 2011 Gator Gazetteabunch9139No ratings yet
- Team Handbook 2011-2-2Document8 pagesTeam Handbook 2011-2-2melissat12785No ratings yet
- Hhs Continue To SoarDocument17 pagesHhs Continue To SoartochumaruNo ratings yet
- 3rd March 2011Document4 pages3rd March 2011ernsteinsNo ratings yet
- Current Grade 5 (SY1314)Document6 pagesCurrent Grade 5 (SY1314)International School ManilaNo ratings yet
- Principal's Message: The Eagle FlyerDocument3 pagesPrincipal's Message: The Eagle Flyerapi-262365902No ratings yet
- E Goshen 12Document2 pagesE Goshen 12api-238851254No ratings yet
- Code of Conduct - 2013-2014 FinalDocument57 pagesCode of Conduct - 2013-2014 Finalapi-248290699No ratings yet
- 2017-2018 HandbookDocument8 pages2017-2018 Handbookapi-289974679100% (1)
- Erie Middle School, Pre AP Focus School: Todd Bissell, Principal Dr. Rachel Heide, Assistant PrincipDocument13 pagesErie Middle School, Pre AP Focus School: Todd Bissell, Principal Dr. Rachel Heide, Assistant PrincipnjtomlinsonNo ratings yet
- Seton Academy Handbook: 23 St. Charles St. Plattsburgh, NY 12901 518-825-7386 518-563-4553 FAXDocument23 pagesSeton Academy Handbook: 23 St. Charles St. Plattsburgh, NY 12901 518-825-7386 518-563-4553 FAXapi-148684093No ratings yet
- Berthoud Eagle: Principal To ParentDocument8 pagesBerthoud Eagle: Principal To ParentRebekah BeckettNo ratings yet
- Erin Margaret Polski: EducationDocument4 pagesErin Margaret Polski: EducationErin SchneiderNo ratings yet
- Third Grade Survival Guide 18-19Document3 pagesThird Grade Survival Guide 18-19api-326382050No ratings yet
- The Buzz at Irmo Middle School: A Special Thank YouDocument4 pagesThe Buzz at Irmo Middle School: A Special Thank YouirmomiddleNo ratings yet
- 1st Grade HandbookDocument8 pages1st Grade Handbookapi-292526984No ratings yet
- 2017 2018 Student Handbook 1Document32 pages2017 2018 Student Handbook 1RAYOU SAONo ratings yet
- Studenthandbook 1415Document59 pagesStudenthandbook 1415api-263051449No ratings yet
- Dixon Elementary Student Handbook 2016-17Document9 pagesDixon Elementary Student Handbook 2016-17bulldogs20130% (1)
- Curriculum Night Second GradeDocument27 pagesCurriculum Night Second Gradeapi-328550972No ratings yet
- 2nd Grade Curriculum Night PresentationDocument15 pages2nd Grade Curriculum Night PresentationChereste Mabra-WestNo ratings yet
- 2016-17 Hae Handbook-2Document8 pages2016-17 Hae Handbook-2api-333215843No ratings yet
- Parent Orientation Powerpoint-2013-2014 PreschoolDocument46 pagesParent Orientation Powerpoint-2013-2014 PreschoolmrfutschNo ratings yet
- Whittier Elementary School Disclosure Document 2014-15Document3 pagesWhittier Elementary School Disclosure Document 2014-15api-239977815No ratings yet
- Duff-Newsome SchoolDocument25 pagesDuff-Newsome Schoolapi-251807548No ratings yet
- Thursday Thoughts: SafetyDocument7 pagesThursday Thoughts: SafetyLaunchpsNo ratings yet
- September Welcome Letter 2013Document5 pagesSeptember Welcome Letter 2013api-252167282No ratings yet
- Thursday Thoughts: Freaky Friday DiscoDocument6 pagesThursday Thoughts: Freaky Friday DiscoLaunchpsNo ratings yet
- High School Newsletter October2Document8 pagesHigh School Newsletter October2api-102758902No ratings yet
- NFPS Information Brochure 2011Document8 pagesNFPS Information Brochure 2011North Fremantle Primary SchoolNo ratings yet
- ViiDocument17 pagesViirutuNo ratings yet
- PreK Parent Handbook 2013-2014Document10 pagesPreK Parent Handbook 2013-20145cr1bdNo ratings yet
- Resume MasterDocument3 pagesResume Masterapi-340262567No ratings yet
- Eagle December 2011 2Document4 pagesEagle December 2011 2cindy_westbrook3178No ratings yet
- Goal 1 Skills Boot Camp Brochure 2Document2 pagesGoal 1 Skills Boot Camp Brochure 2heidihaddadNo ratings yet
- Report Orumana CSDocument11 pagesReport Orumana CSAnonymous dEMsBG100% (1)
- Dear ParentDocument6 pagesDear Parentapi-327986483No ratings yet
- College Admissions at a Glance: Parents' Guide to College AdmissionsFrom EverandCollege Admissions at a Glance: Parents' Guide to College AdmissionsNo ratings yet
- June Lunch 2012Document1 pageJune Lunch 2012dbreynaeNo ratings yet
- Lunch Menu AprilDocument1 pageLunch Menu AprildbreynaeNo ratings yet
- Application 2011 2012Document12 pagesApplication 2011 2012dbreynaeNo ratings yet
- Color Codes July 2012 August 2012 September 2012 October 2012Document5 pagesColor Codes July 2012 August 2012 September 2012 October 2012dbreynaeNo ratings yet
- May Lunch MenuDocument1 pageMay Lunch MenudbreynaeNo ratings yet
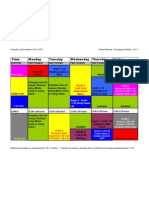
- Computer Lab Schedule 3-12Document1 pageComputer Lab Schedule 3-12dbreynaeNo ratings yet
- Lunch Menu March 2012Document1 pageLunch Menu March 2012dbreynaeNo ratings yet
- Hope Staff 2011-12Document1 pageHope Staff 2011-12dbreynaeNo ratings yet
- Nov. Lunch MenuDocument1 pageNov. Lunch MenudbreynaeNo ratings yet
- Hope Elem Principal's Job Description 2-1-12Document2 pagesHope Elem Principal's Job Description 2-1-12dbreynaeNo ratings yet
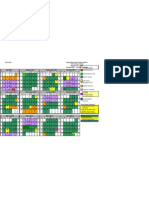
- 2011-2012 CalendarDocument1 page2011-2012 CalendardbreynaeNo ratings yet
- Lunch Menu Jan 2012Document1 pageLunch Menu Jan 2012dbreynaeNo ratings yet
- Application 2011 2012Document12 pagesApplication 2011 2012dbreynaeNo ratings yet
- Hope Staff 2011-12Document1 pageHope Staff 2011-12dbreynaeNo ratings yet
- Lunch Menu MarchDocument1 pageLunch Menu MarchdbreynaeNo ratings yet
- Lunch Menu Feb 2012Document1 pageLunch Menu Feb 2012dbreynaeNo ratings yet
- Lunch Menu JuneDocument1 pageLunch Menu JunedbreynaeNo ratings yet
- Lunch Menu FebDocument1 pageLunch Menu FebdbreynaeNo ratings yet
- Hope Staff Directory 2010-2011Document1 pageHope Staff Directory 2010-2011dbreynaeNo ratings yet
- September Lunch MenuDocument1 pageSeptember Lunch MenudbreynaeNo ratings yet
- September Lunch MenuDocument1 pageSeptember Lunch MenudbreynaeNo ratings yet
- Hope August Lunch MenuDocument1 pageHope August Lunch MenudbreynaeNo ratings yet
- May Lunch MenuDocument1 pageMay Lunch MenudbreynaeNo ratings yet
- Hope August Lunch MenuDocument1 pageHope August Lunch MenudbreynaeNo ratings yet
- April Lunch MenuDocument1 pageApril Lunch MenudbreynaeNo ratings yet
- Hope Elementary 2010-2011 StaffDocument1 pageHope Elementary 2010-2011 StaffdbreynaeNo ratings yet
- Application 2010 2011Document9 pagesApplication 2010 2011dbreynaeNo ratings yet
- Lunch MenuDocument1 pageLunch MenudbreynaeNo ratings yet