You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The A To Z of The Coptic ChurchDocument357 pagesThe A To Z of The Coptic ChurchNoso100% (1)
- Bus 5115 - Discussion Forum Unit 1 University of The PeopleDocument5 pagesBus 5115 - Discussion Forum Unit 1 University of The Peoplechristian allosNo ratings yet
- Weekly Home Learning Plan EditableDocument4 pagesWeekly Home Learning Plan EditableGE-NIAH GEM SALAMANCA100% (1)
- Content Analysis: Objective, Systematic, and Quantitative Description of ContentDocument30 pagesContent Analysis: Objective, Systematic, and Quantitative Description of ContentpratolectusNo ratings yet
- Đề số 01-THI THU 2020Document8 pagesĐề số 01-THI THU 2020mi rrossiNo ratings yet
- Autodesk® Simulation Multiphysics: Course Length: 2 DaysDocument6 pagesAutodesk® Simulation Multiphysics: Course Length: 2 DaysLUISALBERTO06011985No ratings yet
- Angleline and Angle RelationshipsDocument25 pagesAngleline and Angle Relationshipstrtl_1970No ratings yet
- Asanid Ibn JazarizariDocument188 pagesAsanid Ibn Jazarizariseeking knowledgeNo ratings yet
- Jasleen-Resume Dec 62020Document3 pagesJasleen-Resume Dec 62020api-534110108No ratings yet
- Parts of A Persuasive EssayDocument28 pagesParts of A Persuasive EssayHannaNo ratings yet
- Space Curves - 1: Differential Geometry III, Solutions 4 (Week 4)Document3 pagesSpace Curves - 1: Differential Geometry III, Solutions 4 (Week 4)Gag PafNo ratings yet
- The Effect of Leadership Style On Employee Satisfaction andDocument9 pagesThe Effect of Leadership Style On Employee Satisfaction andjrdon123No ratings yet
- Template For Request To Additional Shs Program OfferingDocument7 pagesTemplate For Request To Additional Shs Program OfferingJerome BelangoNo ratings yet
- MidtermDocument3 pagesMidtermapi-272864612No ratings yet
- Clean Edge RazorDocument14 pagesClean Edge RazorOyedele AjagbeNo ratings yet
- Dvar Torah FinalDocument5 pagesDvar Torah FinalKarry TaylorNo ratings yet
- Feasibility Study (Compatibility Mode)Document35 pagesFeasibility Study (Compatibility Mode)Deep ShahNo ratings yet
- 3.1 Thermal PhysicsDocument10 pages3.1 Thermal Physicsmardel11No ratings yet
- DifferentiationsDocument20 pagesDifferentiationsShreyansh KashaudhanNo ratings yet
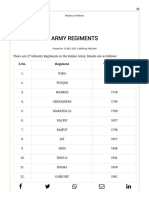
- Army Regiments: S.No. Regiment Year of RaisingDocument3 pagesArmy Regiments: S.No. Regiment Year of RaisingAsc47No ratings yet
- B B A Final - 2Document82 pagesB B A Final - 2sanju377No ratings yet
- Task ManagementDocument11 pagesTask Managementnaveedskhan100% (1)
- Avoiding Shifts in Person, Number and TenseDocument3 pagesAvoiding Shifts in Person, Number and Tenseteachergrace1225No ratings yet
- Di V V: Cardiomath Equations InfoDocument35 pagesDi V V: Cardiomath Equations InfoMd. ashfaque Ahemmed khanNo ratings yet
- QuotessuccessibilityDocument3 pagesQuotessuccessibilityAdrian Julius FloresNo ratings yet
- Mythic Odysseys of Theros (+deluxe Cover) - 2Document26 pagesMythic Odysseys of Theros (+deluxe Cover) - 2gabiNo ratings yet
- Possible Worlds in Narrative SpaceDocument19 pagesPossible Worlds in Narrative SpaceMariia Mandrikova100% (1)
- Intro Pad 101Document43 pagesIntro Pad 101Kemisetso Sadie MosiiwaNo ratings yet
- Anorectal Malformations in A Tertiary Pediatric Surgery Center Fromromania 20 Years of Experience 1584 9341-12-2 3Document5 pagesAnorectal Malformations in A Tertiary Pediatric Surgery Center Fromromania 20 Years of Experience 1584 9341-12-2 3Jeff LapianNo ratings yet
- Stanislavakian Acting As PhenomenologyDocument21 pagesStanislavakian Acting As Phenomenologybenshenhar768250% (2)