Professional Documents
Culture Documents
DOI 2010 Meta-Analysis of Heterogeneous Clinical Trials
DOI 2010 Meta-Analysis of Heterogeneous Clinical Trials
Uploaded by
benjaminsidebotto11Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
DOI 2010 Meta-Analysis of Heterogeneous Clinical Trials
DOI 2010 Meta-Analysis of Heterogeneous Clinical Trials
Uploaded by
benjaminsidebotto11Copyright:
Available Formats
Meta-analysis of heterogeneous clinical trials: An empirical example
Suhail A.R. Doi
a,
, Jan J. Barendregt
b
, Ellen L. Mozurkewich
c
a
Clinical Epidemiology Unit, School of Population Health, University of Queensland, Brisbane, Australia
b
Centre for Burden of Disease and Cost Effectiveness, School of Population Health, University of Queensland, Brisbane, Australia
c
Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, University of Michigan Medical School, Ann Arbor, MI, USA
a r t i c l e i n f o a b s t r a c t
Article history:
Received 17 July 2010
Accepted 6 December 2010
Available online 13 December 2010
Meta-analysis of heterogeneous clinical trials is currently sub-optimal. This is because there has
been no improvement in the method of weighted averaging for such studies since the DL method
in 1986. This article presents the argument for the use of situation specific weights to integrate
results from such trials. An empirical example is given with data from a meta-analysis done
10 years earlier. Previously reported data on 21 studies that looked at the effect of working
conditions onpretermbirths were re-analyzed. Several methods were usedtoestimate the overall
effect sizes. Study specic scores were included in the weighting process when combining studies
and it was shown that this model not only was more conservative than the model of DL but also
retains the legitimacy of the pooledeffect size. The inclusionof appropriate study specic scores in
an appropriate meta-analysis model permits the quantication of the variation between studies
based on something tangible as opposed to the randomadjustments made by the randomeffects
model to the pooled effect size. It is important that such differences are recognized by the wider
research community so that meta-analyses remain a valid tool for synthesizing research.
2010 Elsevier Inc. All rights reserved.
Keywords:
Meta-analysis
Random-effect
Quality-effect
Heterogeneity
Working conditions
1. Introduction
Today, meta-analysis is widely used in a wide range of
disciplines in particular epidemiology and evidence-based
medicine where results of some meta analyses have led to
major changes in clinical practice and health care policies.
Meta-analyses combine the result of several studies that
address a set of related research hypotheses using statistical
methods. The basic hypothesis is that the pooled results from
a group of studies can allow a more accurate estimate of an
effect than an individual study since it overcomes the
problem of reduced statistical power in studies with small
sample sizes.
One problem with meta-analyses today is that differences
between trials, such as sources of bias, are not addressed
appropriately by current meta-analysis models [1]. There are
several reasons for such differences which include chance,
different denitions of treatment effects, credibility related
heterogeneity (quality), and nally unexplainable and real
differences [2]. An important explainable difference is
credibility related heterogeneity (quality) and this refers to
the likelihood of the trial design to generate unbiased results
that are sufciently precise and allow application in clinical
practice [3]. Naturally, the aws in the design of individual
studies will have obvious relevance to creating heterogeneity
between trials as well as an inuence on the magnitude of the
meta-analysis results. If the quality of the primary material is
inadequate, this may falsify the conclusions of the review,
regardless of the presence or absence of effect size hetero-
geneity. The need for addressing heterogeneity in trials via
study specic assessment has been obvious for a long time
and the solution involves more than just inserting a random
termbased on effect size heterogeneity [4] as is done with the
random effects model.
The previous studies [58] that have attempted to
investigate incorporation of some study specic component
in the weighting of the overall estimate concluded that
Contemporary Clinical Trials 32 (2011) 288298
Corresponding author. Clinical Epidemiology Unit, School of Population
Health, University of Queensland, Herston Road, QLD4006, Australia. Tel.: +61
404 181134; fax: +61 7 3365 5599.
E-mail address: sardoi@gmx.net (S.A.R. Doi).
1551-7144/$ see front matter 2010 Elsevier Inc. All rights reserved.
doi:10.1016/j.cct.2010.12.006
Contents lists available at ScienceDirect
Contemporary Clinical Trials
j our nal homepage: www. el sevi er. com/ l ocat e/ concl i nt r i al
incorporating such information into weights provided incon-
sistent adjustment of the estimates of treatment effect. While
these authors follow the same assumption we do that studies
with deciencies are less informative and should have less
inuence on overall outcomes, they focused on individual
studies disregarding the fact that a weight change in one
study impacts all other studies in the meta-analysis. Such
attempts therefore did not reduce bias in the pooled estimate,
and may rather have resulted in an increase in bias.
Recently, a study score adjusted model that overcomes
these limitations has been introduced [9,10]. Our objective
now is to present this quality effects (QE) model that
incorporates study specic scores as weights with consider-
ation of the impact on all studies and compare it to the xed
effects (FE) and random effects (RE) models in a meta-
analysis on working conditions and adverse pregnancy
outcome. We also introduce two important updates to the
QE model as originally published.
2. Rationale
In a group of homogenous trials, it is assumed that because
the effect sizes are homogenous, the studies are all estimating
the same target effect (we can call them type A trials). In this
situation, the inverse variance weights of Woolf [11] will
minimize the variance since:
MSE = Expected EstimateTrue
2
= Variance + Bias
2
:
Bias is zero if the underlying true effect size's are equal and
thus minimizing variance is optimal and the weighted
MSE=Variance. It is thought that this inverse variance
weighted analysis tests the null hypothesis that all studies
in the meta-analysis are identical and show no effect of the
intervention under consideration regardless of homogeneity
[4]. This of course requires the assumption that trials are
exchangeable so that if one large trial is null and multiple
small trials show an effect, the large trial essentially conrms
that the null hypothesis is true. Exchangeability however is a
big assumption and therefore if we do not believe the trials
are exchangeable then in this situation we have two
alternatives: Either the trials have been affected by bias
even though underlying true effects are identical (we can call
these type B trials) or the trials represent different underlying
true effects (we can call these type C trials). In the former
case, the trial effect size from a biased trial might seem like it
is coming from a different underlying true effect, thus giving
the same impression as type C trials: that the trials represent
different underlying true effects. In both types B and C trials,
inverse variance weights will not minimize the variance as it
will just exaggerate and create gross bias in these situations.
Furthermore, any set of weights in a type A situation
estimates the same target, but in a type B or C situation
each set of weights estimates a different target. Thus inverse
variance weights in the latter situation just increases bias and
is not optimal for type B or C trials. Thus in type B or C trials
we would want to use situation specic weights.
One such situation specic weight that has been suggested
for type B trials is weighting according to the probability (Q
i
)
of credibility (internal validity or quality) [810] of the
studies making up the meta-analysis. Although this can
correct for distortions due to systematic error, it can also
introduce errors of another type. For example a study of a
small sample, which is not representative of the underlying
population, may get undeserved weightage from a large
underlying population and this can skew the data. It might
thus be informative to weigh according to precision (inverse
variance) and then re-distribute the weights according to
situation specic requirements. In this case importance of
smaller studies will only get upgraded if the larger or more
precise study is deemed poor by its situation specic weight.
This line of thought is not newas this is precisely what the
random effects model attempts to do [12]. The unfortunate
thing however is that the situation specic weight used in
this particular model is an index of the variability of the effect
sizes across trials and the same situation specic weight is
applied to all trials. This creates two problems, rst that these
weights are meaningless and second that they are not study
specic. In order to rectify this situation, an alternative
approach has been proposed in 2008 [9,10]. In the QE model,
both of the draw-backs of the random model type of re-
distribution have been addressed and an example of this
applied to meta-analysis is provided below.
One further consideration, in type C trials, which deal
usually with burden of disease where true differences across
populations are expected, is the fractional population repre-
sented by the effect size in each study. Of course, a study of, for
example, 1000 respondents is equally useful in examining the
mortality ina country with10 millioninhabitants as it wouldbe
in a country with a population of only 1 million. Without
weighting, any gures that combine data for two or more
countries would over-represent smaller countries at the
expense of larger ones. So a population size weight is needed
to make an adjustment to ensure that each country risk is
represented in the pooled estimate proportional to its
population size. Although such weighting has been attempted
previously, it has been improperly applied [13]. The best
method is to assign a proportional weight between zero and 1
of each study in relation to the largest based on the underlying
population size. The population size weight (Pweight) is thus
the proportional weight Psize
i
/Psize
max
. This corrects for the
fact that most studies may have very similar sample sizes, no
matter how large or small their underlying population. These
weights can be multiplied by internal validity weights (also
between zero and 1) to yield modied internal validity weights
that can then be utilized in the QE model (see Appendix 4).
3. Differences in weighting between models
The standard approach frequently used in meta-analysis in
clinical research is termed the inverse variance method or FE
model based on Woolf [11]. The average effect size across all
studies is computed, whereby the weights are equal to the
inverse variance of each study's effect estimator. Larger studies
andstudies withless randomvariationare givengreater weight
than smaller studies. The weights (w) allocated to each of the
studies are then inversely proportional to the square of the
standard error (se), thus for the ith study
w
i
=
1
se
2
i
289 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
which gives greater weight to those studies with smaller
standard errors.
As can be seen above the variability within each study is
used to weight each studies effect in the current approach to
combining them into a weighted average as this minimizes
the variance (assuming each study is estimating the same
target). So if a study reports a higher variance for its effect size
estimate it would get lesser weight in the nal combined
estimate and vice versa. This approach however does not take
into account the innate variability that exists between the
studies arising from differences inherent to the study such as
their protocols and how well they were executed and
conducted. This major limitation has been well recognized
and it gave rise to the random effects (RE) model approach
[12]. Here, a constant is generated from the homogeneity
statistic Q and using this and other study parameters a
random effects variance component (
2
) is generated. The
inverse of the sampling variance plus this constant that
represents the variability across the population effects is then
used as the weight
w
i
=
1
se
2
i
+
2
where w
i
*
is the random effects weight for the ith study.
However, because of the limitations of the RE model,
when used in a meta-analysis of badly designed studies, it
will still result in biased estimates even though there is
statistical adjustment for effect size heterogeneity [4].
Furthermore, such adjustments, based on an articially
inated variance, lead to a widened condence interval,
supposedly to reect effect size uncertainty, but do not have
much clinical relevance [4,14]. Therefore, a new method for
adjusting for heterogeneity can use situation specic para-
meters and in this case we use study specic scores. These are
then rescaled to a probability Q
i
, the judgement of the
probability (0 to 1) that study i is credible or the proportion
(01) that the underlying study i population makes up of the
largest underlying population of interest and so on. From Q
i
a
study specic composite called
Q
i
is generated that takes into
consideration study specic information and its relationship
to other studies to re-distribute inverse variance weights. As
studies increase in quality or are more representative of the
population, re-distribution becomes progressively less and
ceases when all studies are of perfect quality or representa-
tion. This is totally different from the direct adjustment for
quality of xed effects weights reported by several authors
[5,7,8]. With the QE model, rather than use study specic
scores directly, the composite
Q
i
is generated [10]. The QE
weight, w
i
, is then:
w
i
=
Q
i
w
i
:
Detailed aspects of computation of this model are given in
Appendix 1 with an important update for overdispersion
using a correction factor for individual study variances. A
simulation of 10,000 iterations is detailed in Appendix 2 that
compares the properties of QE and RE models under different
levels of systematic error. This further conrms the validity of
the QE model both under varying levels of between study
differences and in comparison to the RE model.
The extent of redistribution of these weights due to non-
credibility can be assessed via a Q-index dened as follows:
Q =
n
1
1Q
i
w
i
n
1
w
i
_
_
_
_
_
_
_
_
_
_
:
The rationale for this index is that it tells us the probability
that the information contained within the studies in the
meta-analysis is non-credible. The higher the Q-index, the
more likely that the information contained is non-credible
and thus, as Q-index increases, the weights in the meta-
analysis come together and the condence interval of the
pooled estimate increases.
4. Results of application of each of these models
Data from a meta-analysis of 21 studies on the association
of working conditions with preterm birth published between
1983 and 1998 are utilized. The studies were those reported
10 years earlier by Mozurkewich et al. [15]. Each study had
evaluated the effect of working conditions on pretermbirth of
women with a control group. Data abstraction and quality
assessment of each study have previously been reported.
These studies represent a mix of casecontrol, cross-sectional
and retrospective cohorts with large asymmetry between
distribution of individuals in experimental and control arms
and while effect sizes are relatively homogenous, the
included studies are far from homogenous as also indicated
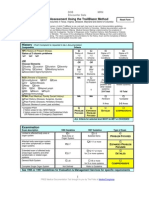
by their distribution of quality scores in Table 1.
The xedeffect (FE) model (inverse variance weighted), the
DerSimonianand Laird's RE method (randomre-distribution of
inverse variance weights) [12] and the Doi and Thalib QE
method (study specic re-distribution of inverse variance
weights) [9,10] were used to calculate the overall effect size.
The quality scores and the effect size estimates of the effect of
working conditions on preterm birth are presented in Table 1,
which also shows the study-specic weights, as a proportion of
the sum of weights, for the xed, random and quality effects
models. We rst showed that since effect size heterogeneity
was minimal (
2
=0.0027), the pooled effect size fromall three
models was comparable. However, because of fairly homoge-
nous effect sizes, QE weighting serves to decrease our
condence in the pooled effect size rather than alter the
estimate of the pooled effect size. Incorporation of the quality
scores was alsoassociatedwitha more conservative condence
interval (1.031.44) thanwiththe REmodel (1.121.3) because
with decreasing effect size heterogeneity, the RE model
approaches the FE model. Differences in weight of individual
studies by QE versus RE model ranges from 18.1 to +3.5%
(Table 1, QE weight minus RE weight). The Q-index was 0.62
suggesting this probability of non-credibility of information
within the studies.
We next explored the impact of changes in the effect size
of the largest study because that is the study with the greatest
impact on a meta-analysis. The rationale for doing this is to
create several levels of effect size heterogeneity. When the
odds ratio (OR) for the largest study (study 9 in Table 1,
N=104,262) was biased to different degrees, there were
290 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
ensuing alterations in the random effects variance compo-
nent (
2
).There was a U shaped relationship between the
2
and the odds ratio with the minimum
2
corresponding to an
OR of 1.24 (Fig. 1) and the randomeffect weight of the largest
study (study 9) had a clear decrease with increasing
2
(Fig. 2). There was no change in the QE weight of study 9 with
increase in heterogeneity of effect sizes (Fig. 2), conrming
that effect size heterogeneity has nothing to do with the way
the QE model's pooled estimate is computed.
The relationship between effect size in the biggest study
and its impact on the pooled RE model effect size is depicted
in Fig. 3. An effect size of 1.24 was associated with the least
effect size heterogeneity (
2
) and thus maximum weight of
study 9 (centre vertical line in Fig. 3). Effect size heteroge-
neity progressively increases on either side of this line with
the weight of study 9 decreasing as heterogeneity increased.
Despite these predictable changes in effect size heterogeneity
Table 1
Data from 21 studies on the effect of working conditions on preterm births in healthy women along with study specic weight for the xed effects, Der Simonian
Laird random effects model and the Doi Thalib quality effects model.
Study Design N
EXP
/N
CONT
Events
E
EXP
/E
CONT
Quality score
(Q
i
)
OR
(95% CI)
w
i
/w
i
(%)
w
i
/w
i
(%)
w
i
/w
i
(%)
Absolute deviation of
OR from median
1 Case control 87/144 25/48 0.57 0.81
(0.451.44)
0.8 1.7 4.2 0.46
2 Cross-sectional 578/1350 47/65 0.42 1.75
(1.182.58)
1.7 3.6 3.4 0.48
3 Retrospective survey 328/1934 20/89 0.33 1.36
(0.832.23)
1 2.3 2.5 0.09
4 Case control 67/291 29/141 0.71 0.81
(0.481.39)
0.9 2 5.3 0.46
5 Cohort 3518/1700 127/56 0.50 1.1
(0.81.51)
2.5 5.2 4.5 0.17
6 Case control 6245/429 579/26 0.50 1.57
(1.052.35)
1.5 3.4 4 0.3
7 Cohort 472/6628 62/746 0.50 1.2
(0.911.58)
3.3 6.7 4.8 0.07
8 Prospective cohort 258/638 15/24 0.42 1.59
(0.823.06)
0.6 1.3 3 0.32
9 Prospective cohort 32,784/
71,478
1836/
3288
0.33 1.23
(1.161.3)
73 42.2 24.1 0.04
10 Cross-sectional 250/624 15/30 0.50 1.27
(0.672.4)
0.6 1.4 3.6 0
11 Cross-sectional 249/286 22/23 0.25 1.11
(0.62.03)
0.7 1.5 1.8 0.16
12 Cross-sectional 2479/1911 131/104 0.50 0.97
(0.741.26)
3.6 7.3 5 0.3
13 Prospective cohort 72/11 5/0 0.50 3.51
(0.06204)
0 0 3.3 2.24
14 Case control 771/699 127/83 0.64 1.46
(1.091.97)
2.8 5.9 6 0.19
15 Prospective cohort 1113/3107 37/121 0.58 0.85
(0.591.24)
1.8 3.9 4.8 0.42
16 Prospective cohort 287/325 32/42 0.33 0.85
(0.521.38)
1.1 2.4 2.5 0.42
17 Cross-sectional 504/1897 71/214 0.50 1.29
(0.971.72)
3 6.3 4.7 0.02
18 Prospective cohort 79/434 3/21 0.58 0.83
(0.252.73)
0.2 0.4 3.9 0.44
19 Retrospective cohort 56/862 5/52 0.25 1.59
(0.624.07)
0.3 0.7 1.7 0.32
20 Prospective cohort 39/1127 9/189 0.42 1.52
(0.713.22)
0.4 1 2.9 0.25
21 Prospective cohort 122/224 9/13 0.58 1.3
(0.543.1)
0.3 0.8 4 0.03
Pooled OR All 1.22
(1.161.28)
1.2
(1.121.3)
1.22
(1.031.44)
OR, Odds Ratio; w
i
, xed effect weight; w
i
, random effects weight, w
i
, quality effects weight.
0
0.01
0.02
0.03
0.04
0.05
0.06
0.8 1 1.2 1.4 1.6
Biased study 9 OR
2
a
f
t
e
r
b
i
a
s
i
n
s
t
u
d
y
9
Fig. 1. Relationship between effect size of the biggest study and Tau squared
in the RE model. Tau squared was recalculated for various biases in the effect
size of study 9 created by varying the experimental group event rate. Tau
squared was minimal at an OR for study 9 of 1.24.
291 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
and study 9 weight, the effect on the pooled effect size was
unpredictable and bore no relationship to the degree of bias
in the effect size of study 9 (Fig. 3).
In the QE model, regardless of what was the extent of the
effect size bias introduced, weight of study 9 remains similar
and therefore the pooled odds ratio for the meta-analysis
under the QE model was also biased in the same direction
(given the high study precision) but only if the study was
deemed to be of good quality (Fig. 4). However, if the
magnitude of the effect size bias is assumed to increase
(irrespective of direction) with decreases in quality, then
there will be minimization of the effect of this bias on the
pooled estimate in the QE model as when the quality of this
study was progressively decreased, the pooled estimate
gradually returned towards the original estimate of an OR
of approximately 1.22 (Fig. 4).
The way the 95% CI of the overall effect size estimate of the
QE model changes with quality is shown in Figs. 5 and 6.
When study 9 is biased to an OR of 0.96, the QE model pooled
estimate was biased in that direction. However, as its quality
of study 9 was decreased, the pooled estimate returned to its
baseline value albeit with a wider condence interval
suggesting that we should have less condence in this pooled
value (Fig. 5). When effect size heterogeneity was minimal
across studies and study 9 was non-biased (Fig. 6), as
credibility of study 9 was decreased, our condence in the
pooled estimate also decreased (wider condence interval),
despite the pooled effect size remaining constant.
Finally, the weight gain (over inverse variance weight) of
the smaller studies that received additional weight in both
the RE and QE models was plotted against a measure of their
heterogeneity. The measure in the RE model was a deviation
of the study effect size from the median and in the QE model
was the probability that the study was credible. The RE re-
distribution bore no relationship to heterogeneity in effect
size (Fig. 7), but the QE model bore a denite linear
relationship to quality (Fig. 8).
5. Discussion
The inclusion of study specic scores in meta-analyses
permits a better understanding of the variation between
studies. The QE method, just described, can be easily applied
and seems to generate more conservative overall estimates
when there is heterogeneity in quality between studies. This
is evident from the fact that the QE summary had a higher
variance and, consequently, wider condence interval than
the RE summary in this meta-analysis. Thus, RE summaries
are not predictably conservative and this has been a problem
even in their relationship to xed effect summaries [16].
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
1.7
1.8
0.7 0.9 1.1 1.3 1.5 1.7
Biased study 9 OR
P
o
o
l
e
d
R
E
M
O
R
a
n
d
9
5
%
C
I
Increasing heterogeneity Increasing heterogeneity
Fig. 3. Relationship between the effect size in the largest study and the
pooled RE model effect size. The pooled RE effect size was recalculated for
various biases in the effect size of study 9 created by varying the
experimental group event rate. The vertical line is the point where tau
squared is minimal and heterogeneity in effect size increases on either side of
the line.
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
0 0.2 0.4 0.6 0.8 1
Quality of study 9
P
o
o
l
e
d
Q
E
M
O
R
OR 0.82
OR 0.96
OR 1.1
OR 1.24
OR 1.38
OR 1.53
OR 1.68
Fig. 4. Relationship between quality of the largest study, its effect size bias
and the pooled QE model effect size. The pooled QE effect size was
recalculated for various biases in the quality of study 9 created by varying
this by 0.1 each time as well as for various biases in the effect size of study 9
created by varying the experimental group event rate. The vertical line
represents the true quality of study 9. Regardless of the direction or
magnitude of the effect size bias, the pooled effect size returned to its original
value when quality decrements were deemed to be associated with
increased effect size bias in study 9.
0.8
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
0.00 0.20 0.40 0.60 0.80 1.00
Probability that study 9 is credible (0-1)
Study 9 OR biased to 0.96
P
o
o
l
e
d
Q
E
M
O
R
a
n
d
9
5
%
C
I
Fig. 5. Relationship between quality and the 95% condence interval of the
QE model pooled effect size when study 9 effect size is biased to 0.96 (OR).
The thin lines are the 95% condence limits on the pooled QE model effect
size (thick line).
0
10
20
30
40
50
0 0.02 0.04 0.06 0.08 0.1
Tau squared
W
e
i
g
h
t
o
f
b
i
g
g
e
s
t
s
t
u
d
y
(
%
)
Fig. 2. Relationship between tau squared and weight allocated to the biggest
study in both the RE and QE models. As tau squared increased, weight
progressively decreased in the RE model (circles) but there was no
signicant impact on the QE model (squares).
292 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
In the RE model, the weight of the larger studies are
redistributed to smaller studies but
2
has a decreasing effect
as study precision declines [14]. The size of
2
is determined
by howheterogeneous the effect sizes are and if
2
is zero, the
RE model defaults to the FE model. If we focus on the largest
study, the bigger its difference from other studies, the bigger
the
2
and the decrease in weight of this study.
2
has a
U-shaped association with effect size in the largest study,
being minimal when the largest study conforms to other
study effect sizes, and as this effect size departs from that of
other studies,
2
increases. The weight of the largest study
then declines as
2
increases. However, while the biggest
individual study weight decrements associated with bigger
2
follow a predictable pattern, the impact of different
2
values
on the pooled estimate is unpredictable. This happens
because while individual study weight changes are predict-
able from
2
, the relationship of weight gain across smaller
studies bears no relationship to which study shows the most
effect size heterogeneity (Fig. 7).
In contrast, with the QE model, the weight of the larger
studies is redistributed to smaller studies only if their
credibility is deemed to be lower. The correction,
i
, is
individualized to each study and increases as study credibility
declines but with an impact proportional to study precision
[9,10]. If
i
is zero for all studies, the QE model defaults to the
FE model. The correction fromone study is redistributed to all
other studies proportional to their credibility. The impact on
the pooled estimate is thus totally driven by what each study
has to offer and maintains a relationship of weight gained
across studies based on heterogeneity in quality (Fig. 8).
If we focus on the largest study again, the bigger its
decrease in credibility, the bigger the penalty applied to this
study by the QE model. Thus a non-credible large study will
not be able to alter estimates of the pooled effect much even if
its effect size is considerably different from the rest of the
studies. But non-credibility also leads to less condence in the
pooled estimate, reected by wider condence intervals. We
have shown in this meta-analysis that if the effect size of the
largest study was biased to an OR of 0.96, the pooled QE
model summary estimate changes in favor of this study only if
its credibility was high. As credibility is decreased the pooled
estimate returns towards its former value. Credibility infor-
mation thus acts as a regulatory mechanism that controls the
impact any one study can have on the pooled estimate.
While this mechanism pre-supposes that non-credibility
leads to bias in the effect-size, this supposition is backed by
clear evidence suggesting that inadequate methodological
reporting correlates with bias in estimation of treatment
effects [1,6,1720]. However, there could be instances where
credibility information does not lead to bias in the estimation
of treatment effects or alternatively where such biases may
have been obscured by the lack of credibility and this meta-
analysis is an example of the latter situation. In such cases, the
QE model is still valid and credibility information results
simply in decreased condence (wider condence intervals)
in the pooled estimate. We do not delete lower quality studies
because every study has something to add to the weighted
estimate and we do not know what the relationship of study
specic scores are to the magnitude nor direction of bias.
However if this weighting is not basedonstudy or goal specic
attributes then the weighted estimate loses meaning. A
sensitivity analysis on the other hand can only tell us that
subgroups are heterogeneous but not what the true estimate
0.9
1
1.1
1.2
1.3
1.4
1.5
1.6
0.00 0.20 0.40 0.60 0.80 1.00
Probability that study 9 is credible (0-1)
Non-biased study 9 OR
P
o
o
l
e
d
Q
E
M
O
R
a
n
d
9
5
%
C
I
Fig. 6. Relationship between quality and the 95% condence interval of the
QE model pooled effect size when study 9 effect size is un-biased. The thin
lines are the 95% condence limits on the pooled QE model effect size (thick
line). As study 9 had minimal effect size heterogeneity, the pooled QE model
effect size did not change with decrements in quality but the condence
interval widened.
0.0
1.0
2.0
3.0
4.0
5.0
0 0.2 0.4 0.6
Deviation of study ES (OR) from the median
A
d
d
i
t
i
o
n
a
l
w
e
i
g
h
t
%
u
n
d
e
r
R
E
m
o
d
e
l
Fig. 7. Relationship between measure of heterogeneity in each study and the
additional weight given (over inverse variance weighting) to each of the
smaller studies under the RE model (study 9 that lost weight was excluded).
Heterogeneity was calculated as the absolute value of the median effect size
across all 21 studies minus the study effect size.
0.0
1.0
2.0
3.0
4.0
5.0
0.20 0.40 0.60 0.80
Probability that study is credible
A
d
d
i
t
i
o
n
a
l
w
e
i
g
h
t
%
u
n
d
e
r
Q
E
m
o
d
e
l
Fig. 8. Relationship between measure of heterogeneity in each study and the
additional weight given (over inverse variance weighting) to each of the
smaller studies under the QE model (study 9 that lost weight was excluded).
Heterogeneity was calculated as the probability that the study was credible.
293 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
is likely to be. In type B studies (systematic error), study
specic scores can lead to the best approximation of the true
effect size while in type C studies (true underlying differ-
ences), using population weights to pool studies can give a
better idea of the population wide estimate. None of these
would be possible with either the RE model or sensitivity
analyses.
While weighting study estimates by their study specic
scores, we must keep in mind that these scores do not tell us
the direction or magnitude of the change in effect size that is
attributable to that score. The QE method of Doi and Thalib
[9], is not constrained by this limitation, because, unlike
previous methods, it does not adjust a study weight directly
but discounts it in relation to all other study weights based on
its quality status. This is exactly what the RE model does too,
the major difference being that the latter adds on weight to
smaller studies without any rationale for doing so and the
process ultimately becomes random. This is because
2
is not
individualized to each study as is
i
in the QE model. This is
demonstrated in Figs. 78 where a gradual increase in weight
of smaller studies with quality is seen but not with effect size
heterogeneity. This also explains why previous attempts to
incorporate study specic scores into weights have failed to
provide sufcient adjustment of the estimates of treatment
effects as they failed to consider heterogeneity individualized
from one study to the next, or worse, even thought of
incorporating study specic scores over the random redistri-
bution in an RE model [5,8].
Greenland suggested more than a decade ago that quality
scoring merges objective information with arbitrary judg-
ments in a manner that can obscure important sources of
heterogeneity among study results [21]. He gave the example
of dietary quality scoring in the Nurses Health Study and states
that the result would likely indicate no diet effects associated
with disease if the effects of important quality items are
confounded within strata of the summary quality score [21].
The problemis to use the information regarding quality in this
way. If we viewedthe diet quality score as the probabilitythat a
Nurses diet is accurately measured (by dividing each score by
the maximumpossible score), we wouldbe able to rank Nurses
by best to worse reliability of dietary information. Even if this
ranking is subjective or poor, we would still be more condent
about diets relationship to disease in high scorers than in low
scorers. This is the correct use of quality scores, but would not
work with conventional meta-analysis models because spread
of precision and effect size take precedence over any
stratication done by quality score [14]. The fact that previous
authors used scores as exclusion criteria or to sequentially
combine trial results using these models would only increase
bias by altering the range of precision and effect size
differences among stratied studies [14]. This is probably
why the reports of stratication of meta-analyses by quality
score report noclear impact onthe pooledestimate [19,2224].
Study specic assessment has not, till now, found an
acceptable means of becoming an important part of meta-
analyses. More than half of published meta-analyses do not
specify in the methods whether and how they would use
study specic assessment in the analysis and interpretation of
results and only about one in a thousand systematic reviews
consider weighting by quality score [25]. This is probably
because of the lack, until now, of an adequate model to do so
and therefore those meta-analyses that had an a priori
conceptualization of quality simply linked it to the interpre-
tation of results or to limit the scope of the review. Although,
there is no gold standard and we still do not knowhowbest to
measure quality, this is not an obstacle to the quality effects
analysis because it works with any quality score [9]. Given
that we have demonstrated that the RE model randomly
adjusts estimates of treatment effects in a meaningless
fashion, it may now be time to switch from observed random
statistical effect size heterogeneity to models that are based
on measured study specic estimates of their heterogeneity.
Appendix 1. The quality effects model computations
The quality adjustor,
i
is given by:
i
=
w
i
w
i
Q
i
N1
where w
i
is the inverse variance weight and Q
i
is the
credibility of study i ranging from zero to 1 and N is the
number of studies in the meta-analysis. This quality adjustor
is then used to compute tau hat. There was a slight error in
the previously published [10] computation of tau hat by the
alternate quality adjustor that allowed in certain situations a
negative weight. This was rectied by computing an adjusted
Q
i
rst as follows:
Q
i
adj =
N
i =1
Q
i
_ _
N
i =1
i
_ _
N1
_
_
_
_
_
_
_
_
_
_
_
_
+ Q
i
if Q
i
Q
i
b 1
Q
i
Otherwise
Tau hat is then given by:
i
=
N
i =1
i
_ _
N
Q
i
adj
N
i =1
Q
i
adj
_
_
_
_
_
_
_
_
_
_
i
:
Tau hat then is used to compute the study specic
variance component Q hat as follows:
Q
i
= Q
i
+
i
w
i
_ _
:
What these equations do is to replace the random effects
variance component with study specic variance components
so that the target this meta-analysis is estimating becomes
meaningful. The nal summary estimate is then given by:
ES
QE
=
w
i
ES
_ _
w
i
=
Q
i
w
i
ES
i
_ _
Q
i
w
i
_ _
where ES is the pooled effect size measure and it has a
variance (v) given by
V
QE
= v
i
w
i
w
i
_ _
2
:
294 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
And thus since w
i
= w
i
Q
i
(where w
i
=
1
v
i
) this reduces to
V
QE
=
Q
2
i
w
i
_ _
Q
i
w
i
_ _ _ _
2
:
However, based on simulation studies, there is signicant
over-dispersion and thus this variance estimate underesti-
mates the true variance and leads to a condence interval
with poor coverage. To rectify this, we added a correction
factor (CF) for over-dispersion based on the Q statistic as
follows:
CF = 1max 0;
Q N1
Q
_ _ _ _
0:25
:
For computation of the variance of the weighted average,
the variance of each study was then inated to the power CF
as follows:
w
i
=
1
v
CF
i
if v
i
b 1 or w
i
=
1
v
2CF
i
if v
i
N 1:
This was then used to compute V
QE
as follows:
V
QE
=
Q
2
i
w
i
_ _
Q
i
w
i
_ _ _ _
2
:
Based on the simulation outlined below in Appendix 2, the
coverage probability of this condence interval is not less than
90% and usually more than the nominal level of 95% for the QE
model even in the presence of substantial heterogeneity.
Assuming the distribution of these estimates is asymptotically
normal, the 95% condence limits are easily obtained by:
95%CI = ES F1:96
v
QE
_
_ _
:
The effect size used in this study was the Ln(OR) with the
se for each study given by:
se =
1
a
+
1
b
+
1
c
+
1
d
_
where a, b, c and d represent the cell counts in a 22 table for
each study. To account for zero outcomes in one of the
studies, a continuity correction was applied by adding 0.5 to
all cell counts [26].
All analyses were done using MetaXL (www.epigear.com)
or an excel spreadsheet available fromthe authors on request.
Appendix 2. Simulation study
This meta-analysis was made up of a fairly homogenous group of studies and thus the comparison above actually compares
essentially a FE and QE model. We therefore decided to simulate what happens when heterogeneity is increased by adding
systematic error to each study. This error needs to be in either direction and of variable magnitude for each study score. We did this
by rst replacing the numbers of events in both arms of the studies by a generation from a binomial distribution with parameters
(N1,p1) and (N2,p2) in the intervention and control arms respectively. N1 and N2 were xed to the same as the original study
data. p2 was generated from a uniform distribution with parameters (0.03, 0.48) which represented the range of control group
event rates in the original meta-analysis. p1 was then computed to deliver an odds ratio of 1.22 which is the odds ratio in the
original QE meta-analysis. This was done by assigning p1 as follows:
p1 =
p2 1:22
1p2 + p2 1:22
:
The standard error (se
i
) for each study thus generated was computed and then inated by a fraction of 0.5 based on each study's
credibility to mimic systematic error as follows:
se
= se
i
+ 0:5 1Q
i
:
A new effect size (LnES
new
) adjusted for systematic error was then generated from a normal distribution with parameters
(Ln1.22, se). P2 generated previously was then used to re-compute p1 that would deliver an odds ratio of exp(LnES
new
) as
follows:
p1
=
p2 exp LnES
new
1p2 + p2 exp LnES
new
:
Anewmeta-analysis was thencomputedwithevents generatedfromabinomial distributionwithparameters (N1,p1) and(N2,p2) in
the intervention and control arms respectively. This meta-analysis was then run 10,000 times using Ersatz simulation software (www.
epigear.com). The simulation was then run two more times, once with decreasing quality with decrease in study size (0.9 for the three
largest studies, then0.8 for the next three andso on) andonce more witha randomnumber betweenzero andone for quality. The results
comparing the QE and RE models are given in the tables below.
295 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
Appendix 3. Overdispersion correction
In a study with overdispersed data, the mean or
expectation structure () is adequate but the variance
structure [
2
()] is inadequate. Individuals in the study can
have the outcome with some degree of dependence on study
specic parameters unrelated to the intervention. If such data
are analyzed as if the outcomes were independent, then
sampling variances tend to be too small giving a false sense of
precision. One approach is to think of the true variance
structure as following the form [()
2
()]; however it is
complex to t such a form. As a simpler approach we suppose
()=c, so that the true variance structure [c
2
()] is some
constant multiplier of the theoretical variance structure. A
common method of estimating c is to use the observed chi
squared goodness of t statistic for the pooled studies divided
by its degrees of freedom [2729]:
c =
2
= df:
If there is no overdispersion or lack of t, c=1 (because
the expected value of the chi squared statistic is equal to its
degrees of freedom) and if there is then cN1. In a meta-
analysis this goodness of t chi squared divided by its df is
equal to H
2
as dened by Higgins [30].
The problem of using the overdispersion parameter as a
constant multiplier of the variances of each study in the meta-
analysis presupposes that for a constant increase in this
parameter, there is a constant increase in variance. This
means that the impact of the parameter is not capped and a
Appendix Table S2.1
Results of 10,000 simulations using original quality scores. True underlying effect size was 1.22.
Parameter QE results RE results
Coverage probability of the condence interval 99.3% 88.1%
Mean pooled estimate (95% CI)
Range
1.237 (1.2321.239)
0.711.94
1.252 (1.2491.254)
0.841.91
Median variance (IQR)
Range
0.033 (0.0170.054)
0.00390.414
0.007 (0.00530099)
0.00120.043
Pooled effect size N1.12 and b1.32 44.97% 55.8%
Pooled effect size b1 6.7% 1.51%
Pooled effect size N1.5 6.8% 3.3%
Median Tau squared (IQR)
Range
0.105 (0.0730.158)
0.00680.825
Median Q-index (IQR) 0.63 (0.620.64)
Appendix Table S2.2
Results of 10,000 simulations using greater quality for bigger studies. True underlying effect size was 1.22.
Parameter QE results RE results
Coverage probability of the condence interval 95.5% 86.4%
Mean pooled estimate (95% CI)
Range
1.22 (1.2241.226)
1.01.48
1.25 (1.2481.252)
0.891.76
Median variance (IQR)
Range
0.0034 (0.00240.0047)
0.00260.0329
0.0036 (0.00290.0044)
0.00340.011
Pooled effect size N1.12 and b1.32 87.28% 69.01%
Pooled effect size b1 0% 0.27%
Pooled effect size N1.5 0% 1.04%
Median Tau squared (IQR)
Range
0.042 (0.0310.055)
00.175
Median Q-index (IQR) 0.13 (0.1290.146)
Appendix Table S2.3
Results of 10,000 simulations using random quality scores. True underlying effect size was 1.22.
Parameter QE results RE results
Coverage probability of the condence interval 99.2% 87.7%
Mean pooled estimate (95% CI)
Range
1.230 (1.2281.233)
0.732.03
1.252 (1.2491.254)
0.871.85
Median variance (IQR)
Range
0.0272 (0.0150.049)
0.00040.7196
0.0067 (0.00490093)
0.00080.0679
Pooled effect size N1.12 and b1.32 56.75% 56.68%
Pooled effect size b1 4.19% 1.4%
Pooled effect size N1.5 4.04% 3.59%
Median Tau squared (IQR)
Range
0.097 (0.0640.148)
0.0031.35
Median Q-index (IQR) 0.499 (0.320.686)
296 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
point is eventually reached where there is over-ination of
the variances for a given level of overdispersion resulting in
overcorrection and condence intervals that are too wide. In
order to reduce the impact of large values of H
2
we can
transform H
2
to its reciprocal and use this to proportionally
inate the variances. Interestingly, Higgins [30] has also
dened an I
2
parameter, which is an index of dispersion that
is restricted between zero (no dispersion) and 1. If we reverse
the I
2
scale (by subtracting it from 1) so that no dispersion
(only sampling error) is now 1 as opposed to zero, then
(1I
2
) is indeed the reciprocal of H
2
. We thus used (1I
2
) as
an exponent to proportionally inate study variances b1. For
variance N1, we used 2 minus this overdispersion parameter
(which reduces to [I
2
+1]) as the ination factor. Additional
re-scaling was done by scaling (1I
2
) to various roots and
using the simulation described above to see the impact on
coverage of the condence interval. The fourth root was
found to result in an acceptable simulated coverage of the
condence interval around 95%. We thus used [(1I
2
)
1/4
] as
the nal overdispersion correction factor. This is also
equivalent to (1/H
2
)
1/4
. This correction was then used to
inate the variances of individual studies resulting in a more
conservative meta-analysis pooled variance. Even if the
accuracy of this approximation is questionable, common
sense suggests that it is better to perform this correction,
implicitly making the (more or less incorrect) assumption
that the distribution of c is approximated well enough by a
2
-distribution with k1 degrees of freedom than not to
perform any correction at all, implicitly making the (certainly
incorrect) assumption that there is no overdispersion in the
data [28]. Finally, it must be pointed out that this adjustment
in the QE model corrects for overdispersion within studies
that affect the precision of the pooled estimate, not for
heterogeneity between studies that affect the estimate itself.
Appendix 4. Quality scores and population impact scores
For a quality effects type of meta-analysis, a reproducible, and effective scheme of quality assessment is required. However, any
quality score can be used with the method and thus we are not constrained to any one method. The scheme we used in the meta-
analysis that we report here was actually the same used in the original meta-analysis and adapted from criteria for quality
evaluation of the internal validity of observational studies dened by Realini and Goldzieher [31]. After study-specic
modication, this system allowed a maximum overall score of 14 for casecontrol studies and 12 for other observational study
designs (cross-sectional studies, prospective and retrospective cohorts). For casecontrol studies, 02 points were assigned based
on each of 7 components:
1) predetermined method for selection of cases and controls,
2) dened work-related exposure ,
3) unbiased data collection,
4) equivalent patient recall (anamnestic equivalence)
5) exclusions unlikely to create bias (avoidance of constrained cases and controls)
6) equal demographic susceptibility and
7) equal clinical susceptibility.
For cohort and cross-sectional studies, 02 points were assigned for each of six parameters which included:
1) equal demographic susceptibility,
2) equal clinical susceptibility
3) adherence monitoring,
4) analysis of dropouts,
5) representativeness of population and
6) prospective versus retrospective cohort.
There are many different quality assessment instruments and most have got parameters that allow us to assess the likelihood
for bias. While there are many different items that relate to study quality, in an attempt to standardize these a Delphi method has
been used [32]. This is so called because the 206 items associated with study quality that were initially listed were reduced to nine
by means of the Delphi consensus technique. This scheme seeks to assess three dimensions of the quality of studies (internal
validity, external validity and statistical analysis), and focuses on experimental trials. Although the importance of such quality
assessment of experimental studies is well established, quality assessment of other study designs in systematic reviews is far less
well developed [33]. The feasibility of creating one quality checklist to apply to various study designs has been explored [34], and
research has gone into developing an instrument to measure the methodological quality of observational studies [35], and a scale
to assess the quality of observational studies in meta-analyses [36]. Nevertheless, there is as yet no consensus on howto synthesize
information about quality from a range of study designs within a systematic review. We now know that a more balanced view of
observational and experimental evidence is necessary [37], and therefore we proposed previously [9] a combination of the
NewcastleOttawa quality assessment scale for observational studies and the Delphi model for experimental studies as a possible
step forwards. The way Q
i
is computed from the score for each study and the additional use of population weights (for burden of
disease studies) is depicted in the table below.
297 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
References
[1] Conn VS, Rantz MJ. Research methods: managing primary study quality
in meta-analyses. Res Nurs Health 2003;26(4):32233.
[2] Bailey KR. Inter-study differences: how should they inuence the
interpretation and analysis of results? Stat Med 1987;6(3):35160.
[3] Verhagen AP, de Vet HC, de Bie RA, Boers M, van den Brandt PA. The art
of quality assessment of RCTs included in systematic reviews. J Clin
Epidemiol 2001;54(7):6514.
[4] Senn S. Trying to be precise about vagueness. Stat Med 2007;26(7):
141730.
[5] Berard A, Bravo G. Combining studies using effect sizes and quality
scores: application to bone loss in postmenopausal women. J Clin
Epidemiol 1998;51(10):8017.
[6] Moher D, Pham B, Jones A, et al. Does quality of reports of randomised
trials affect estimates of intervention efcacy reported in meta-
analyses? Lancet 1998;352(9128):60913.
[7] Leeang M, Reitsma J, Scholten R, et al. Impact of adjustment for quality
on results of metaanalyses of diagnostic accuracy. Clin Chem 2007;53
(2):16472.
[8] Tritchler D. Modelling study quality in meta-analysis. Stat Med 1999;18
(16):213545.
[9] Doi SA, Thalib L. A quality-effects model for meta-analysis. Epidemiology
2008;19(1):94100.
[10] Doi SA, Thalib L. An alternative quality adjustor for the quality effects
model for meta-analysis. Epidemiology 2009;20(2):314.
[11] Woolf B. On estimating the relation between blood group and disease.
Ann Hum Genet 1955;19(4):2513.
[12] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin
Trials 1986;7(3):17788.
[13] BathamA, Gupta MA, Rastogi P, et al. Calculating prevalence of hepatitis
B in India: using population weights to look for publication bias in
conventional meta-analysis. Indian J Pediatr 2009;76(12):124757.
[14] Al Khalaf MM, Thalib L, Doi SA. Combining heterogenous studies using
the 724 random-effectsmodel is amistake and leads to inconclusive
meta-analyses. J Clin Epidemiol 2011;64(2):11923.
[15] Mozurkewich EL, Luke B, Avni M, Wolf FM. Working conditions and
adverse pregnancy outcome: a meta-analysis. Obstet Gynecol 2000;95
(4):62335.
[16] Poole C, Greenland S. Random-effects meta-analyses are not always
conservative. Am J Epidemiol 1999;150(5):46975.
[17] Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias.
Dimensions of methodological quality associated with estimates of
treatment effects in controlled trials. JAMA 1995;273(5):40812.
[18] Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and
discrepancies between large and small randomized trials in meta-analyses.
Ann Intern Med 2001;135(11):9829.
[19] Balk EM, Bonis PA, Moskowitz H, et al. Correlation of quality measures
with estimates of treatment effect in meta-analyses of randomized
controlled trials. JAMA 2002;287(22):297382.
[20] Egger M, Juni P, Bartlett C, Holenstein F, Sterne J. How important are
comprehensive literature searches and the assessment of trial quality in
systematic reviews? Empirical study. Health Technol Assess 2003;7(1):
176.
[21] Greenland S. Invited commentary: a critical look at some popular meta-
analytic methods. Am J Epidemiol 1994;140(3):2906.
[22] Herbison P, Hay-Smith J, Gillespie WJ. Adjustment of meta-analyses on
the basis of quality scores should be abandoned. J Clin Epidemiol
2006;59(12):124956.
[23] Juni P, Witschi A, Bloch R, Egger M. The hazards of scoring the quality of
clinical trials for meta-analysis. JAMA 1999;282(11):105460.
[24] Whiting P, Harbord R, Kleijnen J. No role for quality scores in systematic
reviews of diagnostic accuracy studies. BMC Med Res Methodol 2005;5:
19.
[25] Moja LP, Telaro E, D'Amico R, et al. Assessment of methodological
quality of primary studies by systematic reviews: results of the
metaquality cross sectional study. BMJ 2005;330(7499):1053.
[26] Sweeting MJ, Sutton AJ, Lambert PC. What to add to nothing? Use and
avoidance of continuity corrections in meta-analysis of sparse data. Stat
Med 2004;23(9):135175.
[27] McCullagh P, Nelder JA. Generalized linear models. London: Chapman &
Hall; 1983. edn.
[28] Tjur T. Nonlinear regression, quasi likelihood, and overdispersion in
generalized linear models. Am Stat 1998;52(3):2227.
[29] Lindsey JK. On the use of corrections for overdispersion. Appl Stat
1999;48:55361.
[30] Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis.
Stat Med 2002;21(11):153958.
[31] Realini JP, Goldzieher JW. Oral contraceptives and cardiovascular
disease: a critique of the epidemiologic studies. Am J Obstet Gynecol
1985;152(6 Pt 2):72998.Notes: GENERAL NOTE: PIP: TJ: AMERICAN
JOURNAL OF OBSTETRICS AND GYNECOLOGY.
[32] Verhagen AP, de Vet HC, de Bie RA, et al. The Delphi list: a criteria list for
quality assessment of randomized clinical trials for conducting
systematic reviews developed by Delphi consensus. J Clin Epidemiol
1998;51(12):123541.
[33] Deeks JJ, Dinnes J, D'Amico R, et al. Evaluating non-randomised
intervention studies. Health Technol Assess 2003;7(27):1173 iiix.
Notes: CORPORATE NAME: International Stroke Trial Collaborative
Group CORPORATE NAME: European Carotid Surgery Trial Collabora-
tive Group.
[34] Downs SH, Black N. The feasibility of creating a checklist for the
assessment of the methodological quality both of randomised and non-
randomised studies of health care interventions. J Epidemiol Community
Health 1998;52(6):37784.
[35] SlimK, Nini E, Forestier D, et al. Methodological index for non-randomized
studies (minors): development and validation of a newinstrument. ANZ J
Surg 2003;73(9):7126.
[36] Wells G, Shea B, O'Connell D, et al. The NewcastleOttawa Scale (NOS)
for assessing the quality of nonrandomised studies in meta-analyses.
http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm2007
last accessed 15th June.
[37] Concato J. Observational versus experimental studies: what's the
evidence for a hierarchy? NeuroRx 2004;1(3):3417.
Table S4.1
Hypothetical calculation of Q
i
for use in QE meta-analyses.
a
Study name Points assigned
based on quality
checklist (maximum
possible eg12 points)
Probability that
study is credible
(Qi)
Population at risk
(if applicable and only
for burden of disease
studies)
Population weight Modified Qi based on
population weight
Study A 5 5/12 = 0.42 100,000 100,000/400,000 =
0.25
0.42 0.25 = 0.1
Study B 7 7/12 = 0.58 400,000 400,000/400,000 =
1
0.58 1 = 0.58
Study C 10 10/12 = 0.83 200,000 200,000/400,000 =
0.5
0.83 0.5 = 0.42
a
Shaded portions only in burden of disease (type C) studies.
298 S.A.R. Doi et al. / Contemporary Clinical Trials 32 (2011) 288298
You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Trailblazer Medicare Audit ToolDocument4 pagesTrailblazer Medicare Audit Tooladultmedicalconsultants100% (10)
- BPQ Questionnaire PDFDocument4 pagesBPQ Questionnaire PDFAymen DabboussiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Barriers To EbpDocument47 pagesBarriers To Ebpvallal100% (1)
- International Aquafeed - May - June 2016 FULL EDITIONDocument80 pagesInternational Aquafeed - May - June 2016 FULL EDITIONInternational Aquafeed magazineNo ratings yet
- Executive Order - BeswmcDocument3 pagesExecutive Order - BeswmcChristopher Torres85% (26)
- CIS Yuva Bharat Health PolicyDocument7 pagesCIS Yuva Bharat Health PolicyS PNo ratings yet
- History of Physical TherapyDocument11 pagesHistory of Physical Therapyapi-271035341No ratings yet
- Literature ReviewDocument4 pagesLiterature Reviewapi-549799448No ratings yet
- Changes in Adolescents Health 7Document2 pagesChanges in Adolescents Health 7Cristine Joy GardoceNo ratings yet
- Tretman Otpadnih Voda Zenice - MesicDocument9 pagesTretman Otpadnih Voda Zenice - MesicNarcisNo ratings yet
- File Ibu LiaDocument710 pagesFile Ibu LiaArum Nadia HafifiNo ratings yet
- Visitacion Act 1 Tdee Stats ReportDocument3 pagesVisitacion Act 1 Tdee Stats ReportHannah VisitacionNo ratings yet
- Labyrinth It IsDocument45 pagesLabyrinth It IsNana OkujavaNo ratings yet
- Diease LossDocument10 pagesDiease LossGeetha EconomistNo ratings yet
- Commentary: Dr. Brian BudgellDocument6 pagesCommentary: Dr. Brian Budgellsolstar1008No ratings yet
- S - Lession of The Infratemporal Fossa and Parapharyngeal Region, Congenital and Developmental Anomalies - RGDocument38 pagesS - Lession of The Infratemporal Fossa and Parapharyngeal Region, Congenital and Developmental Anomalies - RGanon_744980746No ratings yet
- Ce Registtration CertDocument306 pagesCe Registtration CertMuhammad usman khalidNo ratings yet
- SHAHRANIDocument6 pagesSHAHRANIMishellKarelisMorochoSegarraNo ratings yet
- YBP327 MatKool Media BriefDocument2 pagesYBP327 MatKool Media BriefAngel PigNo ratings yet
- Full Spectrum Health, LLC: 307 E Northern Lights, Ste 201 Anchorage, AK 99503:: 907-229-9766Document4 pagesFull Spectrum Health, LLC: 307 E Northern Lights, Ste 201 Anchorage, AK 99503:: 907-229-9766Tracey WieseNo ratings yet
- Ahme Paper RevisedDocument54 pagesAhme Paper Revisedkassahun meseleNo ratings yet
- Human Spinal Cord Picture C1 To S5 VertebraDocument3 pagesHuman Spinal Cord Picture C1 To S5 Vertebraajjju02No ratings yet
- Earth Essence CBD GummiesDocument6 pagesEarth Essence CBD GummiesketsaadanNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz Results Experiment ResultsDocument4 pagesPhysioex Lab Report: Pre-Lab Quiz Results Experiment ResultscharessaNo ratings yet
- Factors Associated With Compassion Satisfaction, Burnout, andDocument30 pagesFactors Associated With Compassion Satisfaction, Burnout, andpratiwi100% (1)
- Trichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCDocument27 pagesTrichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCsushma shresthaNo ratings yet
- Why Do We Believe in Conspiracy Theories?Document6 pagesWhy Do We Believe in Conspiracy Theories?Tony A. SnmNo ratings yet
- Biology 2 JournalDocument5 pagesBiology 2 JournalKadymars JaboneroNo ratings yet
- StarHealthAssureInsurancePolicy ProposalFormDocument4 pagesStarHealthAssureInsurancePolicy ProposalFormshirishkanhegaonkar2No ratings yet
- Febrile Seizure CPGDocument7 pagesFebrile Seizure CPGLM N/ANo ratings yet