You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Nokia 5800xm Rm-356 Rm-427 Service Schematics v2Document8 pagesNokia 5800xm Rm-356 Rm-427 Service Schematics v2Fernan Alvarino SarmientoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Cancer Survivor's Guide - Foods That Help You Fight BackDocument258 pagesCancer Survivor's Guide - Foods That Help You Fight BackVegan Future100% (8)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Barre Lieou SindromDocument1 pageBarre Lieou SindromAmiablePCNo ratings yet
- Raidmax AtlasDocument1 pageRaidmax AtlasAmiablePCNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Barre Lieou SindromDocument1 pageBarre Lieou SindromAmiablePCNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Fibroscan 01Document8 pagesFibroscan 01AmiablePCNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Windows 8 Global ShortcutsDocument2 pagesWindows 8 Global ShortcutsAmiablePCNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Salus RT500RF ManualDocument28 pagesSalus RT500RF ManualAmiablePCNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Cache Memory: Maninder KaurDocument18 pagesCache Memory: Maninder KaurMisha AnonyNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Page 1Document804 pagesPage 1H Aries OñaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MSP430 C Compiler Programming GuideDocument242 pagesMSP430 C Compiler Programming Guidecharles_sieNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- LinuxDocument24 pagesLinuxMaxNo ratings yet
- Linux Configuration FilesDocument5 pagesLinux Configuration FilesSanojNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Pastoral TheologyDocument4 pagesPastoral TheologyIlli KrineisNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- READING DIAG WORD David TrejoDocument3 pagesREADING DIAG WORD David TrejoDavid TrejoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Network Monitoring With ZabbixDocument6 pagesNetwork Monitoring With ZabbixGustavo Sánchez CotoNo ratings yet
- Slang Expressions and ColloquialismsDocument1 pageSlang Expressions and ColloquialismsAhcel Ortiz SomodioNo ratings yet
- Roberto ClementeDocument1 pageRoberto Clementeapi-293783723No ratings yet
- Detailed Lesson Plan GR7Document4 pagesDetailed Lesson Plan GR7Karen VenturaNo ratings yet
- Manual Ricoh Aficio MP C2500Document6 pagesManual Ricoh Aficio MP C2500Compu Red ExpresNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
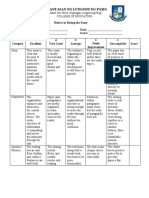
- 5rubric in Rating An EssayDocument3 pages5rubric in Rating An EssayAndy GlovaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Clock Gear Calculator InstructionsDocument2 pagesClock Gear Calculator InstructionsDaksh Dhingra0% (1)
- Latihan Soal On Line Kls 4Document4 pagesLatihan Soal On Line Kls 4Sumiyah CummyNo ratings yet
- QI: Short Answer Questions: 4 7 28Document6 pagesQI: Short Answer Questions: 4 7 28aos tpvNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- UntitledDocument18 pagesUntitledhusamNo ratings yet
- Fox and Mcdonalds Introduction To Fluid Mechanics 8th Edition Pritchard Solutions Manual 2Document2 pagesFox and Mcdonalds Introduction To Fluid Mechanics 8th Edition Pritchard Solutions Manual 2dextrermachete4amgqgNo ratings yet
- Teacher's Resource Book Wonder 6Document129 pagesTeacher's Resource Book Wonder 6izasbj70% (23)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Excel Grade 5 LessPlans Mod 3Document24 pagesExcel Grade 5 LessPlans Mod 3Narine HovhannisyanNo ratings yet
- Farewell Song Lyrics Ryoko MoriyamaDocument1 pageFarewell Song Lyrics Ryoko MoriyamaTim MinNo ratings yet
- Avoid truncating enterprise attributes in incremental loadsDocument7 pagesAvoid truncating enterprise attributes in incremental loadsAnonymous FtmFHWBCs5No ratings yet
- Ic 05Document11 pagesIc 05Luvie Jhun GahiNo ratings yet
- Lkc-Fes Y1S3 L1 Ms. Tan Jue XinDocument3 pagesLkc-Fes Y1S3 L1 Ms. Tan Jue XinXin HuiNo ratings yet
- Resources For Teachers TKT ClilDocument4 pagesResources For Teachers TKT ClilRachel Maria RibeiroNo ratings yet
- Job Opportunities After Post Graduate Diploma in Advanced Computing (PG-DAC)Document2 pagesJob Opportunities After Post Graduate Diploma in Advanced Computing (PG-DAC)Roman PeirceNo ratings yet
- ESL Lesson PlanDocument4 pagesESL Lesson PlanRalph Julius DomingoNo ratings yet
- Infinitivi, Gerund, ParticipiDocument6 pagesInfinitivi, Gerund, ParticipiMartinaNo ratings yet
- Subject Name: Bangladesh Studies Subject Code: 110: Assignment On: 01Document30 pagesSubject Name: Bangladesh Studies Subject Code: 110: Assignment On: 01Ibrahimkholil2011No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)