You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Complete Hemi Sync Gateway Experience ManualDocument43 pagesComplete Hemi Sync Gateway Experience Manualapi-385433292% (92)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Module 4-Answer KeyDocument100 pagesModule 4-Answer KeyAna Marie Suganob82% (22)
- Hotel Design Planning and DevelopmentDocument30 pagesHotel Design Planning and DevelopmentTio Yogatma Yudha14% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Oracle Fusion Financials Book Set Home Page SummaryDocument274 pagesOracle Fusion Financials Book Set Home Page SummaryAbhishek Agrawal100% (1)
- Assignment 3 Part 3 PDFDocument6 pagesAssignment 3 Part 3 PDFStudent555No ratings yet
- Trove Research Carbon Credit Demand Supply and Prices 1 June 2021Document51 pagesTrove Research Carbon Credit Demand Supply and Prices 1 June 2021Ceren ArkancanNo ratings yet
- Pope Francis's Message To Eurojam 2014Document2 pagesPope Francis's Message To Eurojam 2014EddieNo ratings yet
- Eagle Scouts - Merit Beyond The Badge - 210-045 - WBDocument77 pagesEagle Scouts - Merit Beyond The Badge - 210-045 - WBEddie100% (1)
- The Eagle Scout Court of Honor HandbookDocument102 pagesThe Eagle Scout Court of Honor HandbookEddie100% (1)
- M8.2 Offshore Northern Chile Earthquake of 1 April 2014Document1 pageM8.2 Offshore Northern Chile Earthquake of 1 April 2014EddieNo ratings yet
- Bsa 2014 NamDocument1 pageBsa 2014 NamEddieNo ratings yet
- FCSS Activities Calendar 2014.Document1 pageFCSS Activities Calendar 2014.EddieNo ratings yet
- Christian Mission and Education Through Scouting ICCS 2010Document65 pagesChristian Mission and Education Through Scouting ICCS 2010EddieNo ratings yet
- FIPL PoliticoAd l3-11Document1 pageFIPL PoliticoAd l3-11EddieNo ratings yet
- Morgan Weed: Servant Leader in ActionDocument8 pagesMorgan Weed: Servant Leader in ActionMarty B. TschetterNo ratings yet
- CICS Interreligious Dialogue 2007Document100 pagesCICS Interreligious Dialogue 2007EddieNo ratings yet
- UIGSE-FSE Vademecum For International RelationshipsDocument10 pagesUIGSE-FSE Vademecum For International RelationshipsEddieNo ratings yet
- EU CoordEx 2014 FINLANDDocument5 pagesEU CoordEx 2014 FINLANDEddieNo ratings yet
- OCHA UN-CMCoord 2014 Calendar of EventsDocument1 pageOCHA UN-CMCoord 2014 Calendar of EventsEddieNo ratings yet
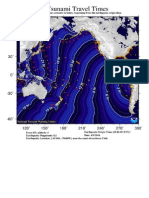
- Chile: Tsunami Travel Times (1 April 2014)Document1 pageChile: Tsunami Travel Times (1 April 2014)EddieNo ratings yet
- Fallo de La Haya: Este Es El DocumentoDocument71 pagesFallo de La Haya: Este Es El DocumentoLa RepúblicaNo ratings yet
- WOSM Constitution enDocument19 pagesWOSM Constitution ensoul_xathiNo ratings yet
- Sofex 2014Document15 pagesSofex 2014EddieNo ratings yet
- Putting Down Roots So Cal 2011Document32 pagesPutting Down Roots So Cal 2011judy_cNo ratings yet
- EMS Systems in The EUDocument96 pagesEMS Systems in The EUEddie0% (1)
- Meridian 13 Fall MRA 2013Document16 pagesMeridian 13 Fall MRA 2013EddieNo ratings yet
- Philmont75 Jul - Aug 2013Document1 pagePhilmont75 Jul - Aug 2013EddieNo ratings yet
- NZSAR Link 24 - September 2013Document12 pagesNZSAR Link 24 - September 2013EddieNo ratings yet
- Jamboree 2013 Staff Guide - The Summit - Boy Scouts of AmericaDocument27 pagesJamboree 2013 Staff Guide - The Summit - Boy Scouts of AmericaEddieNo ratings yet
- IKAR-CISA 2013 Terrestrial Rescue ReportDocument10 pagesIKAR-CISA 2013 Terrestrial Rescue ReportEddieNo ratings yet
- Merit Badge Counselor 220-060Document2 pagesMerit Badge Counselor 220-060EddieNo ratings yet
- U.S. Department of The Army Personal Policy Guidance For Overseas Contingency Operations 1 July 2009 2 November 2011Document210 pagesU.S. Department of The Army Personal Policy Guidance For Overseas Contingency Operations 1 July 2009 2 November 2011Eddie100% (1)
- Asperges MeDocument1 pageAsperges MeEddieNo ratings yet
- Merit Badge Counselor 18-125Document2 pagesMerit Badge Counselor 18-125EddieNo ratings yet
- ISIC Rev.4 International Standard Industrial Classification of All Economic Activities, Rev.4 - EnglishDocument306 pagesISIC Rev.4 International Standard Industrial Classification of All Economic Activities, Rev.4 - EnglishEddie100% (2)
- TCCC Guidelines September 2012Document14 pagesTCCC Guidelines September 2012Valentin GlezNo ratings yet
- Exam Ref AZ 305 Designing Microsoft Azure Infrastructure Sol 2023Document285 pagesExam Ref AZ 305 Designing Microsoft Azure Infrastructure Sol 2023maniNo ratings yet
- EE-434 Power Electronics: Engr. Dr. Hadeed Ahmed SherDocument23 pagesEE-434 Power Electronics: Engr. Dr. Hadeed Ahmed SherMirza Azhar HaseebNo ratings yet
- STERNOL Specification ToolDocument15 pagesSTERNOL Specification ToolMahdyZargarNo ratings yet
- 01 Design of Flexible Pavement Using Coir GeotextilesDocument126 pages01 Design of Flexible Pavement Using Coir GeotextilesSreeja Sadanandan100% (1)
- 277Document18 pages277Rosy Andrea NicolasNo ratings yet
- Accidental PoisoningDocument3 pagesAccidental PoisoningBRUELIN MELSHIA MNo ratings yet
- Rakpoxy 150 HB PrimerDocument1 pageRakpoxy 150 HB Primernate anantathatNo ratings yet
- 67c Series Bulletin 08 04 PDFDocument12 pages67c Series Bulletin 08 04 PDFnight wolfNo ratings yet
- Brooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFDocument36 pagesBrooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFlois.guzman538100% (12)
- EPF Passbook Details for Member ID RJRAJ19545850000014181Document3 pagesEPF Passbook Details for Member ID RJRAJ19545850000014181Parveen SainiNo ratings yet
- Voltaire's Candide and the Role of Free WillDocument3 pagesVoltaire's Candide and the Role of Free WillAngy ShoogzNo ratings yet
- Quality CircleDocument33 pagesQuality CircleSudeesh SudevanNo ratings yet
- StsDocument10 pagesStsSamonte, KimNo ratings yet
- Front Cover Short Report BDA27501Document1 pageFront Cover Short Report BDA27501saperuddinNo ratings yet
- E Learning: A Student Guide To MoodleDocument16 pagesE Learning: A Student Guide To MoodleHaytham Abdulla SalmanNo ratings yet
- Agricultural Sciences P1 Nov 2015 Memo EngDocument9 pagesAgricultural Sciences P1 Nov 2015 Memo EngAbubakr IsmailNo ratings yet
- C ClutchesDocument131 pagesC ClutchesjonarosNo ratings yet
- The Emperor Jones: What's Inside in ContextDocument27 pagesThe Emperor Jones: What's Inside in ContextHarshvardhan RaiNo ratings yet
- Practical LPM-122Document31 pagesPractical LPM-122anon_251667476No ratings yet
- Kastanakis 2014Document8 pagesKastanakis 2014Andreea Georgiana MocanuNo ratings yet
- Genre Worksheet 03 PDFDocument2 pagesGenre Worksheet 03 PDFmelissaNo ratings yet
- Plant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirDocument20 pagesPlant Air Centrifugal Compressors: Turbo-Air Series Featuring Oil-Free AirSharad KokateNo ratings yet
- Ne 01 20 09 2018Document436 pagesNe 01 20 09 2018VaradrajNo ratings yet