You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Micro Exam Topics 2012Document1 pageMicro Exam Topics 2012Frankie LiuNo ratings yet
- Integ Activity 2012Document15 pagesInteg Activity 2012Frankie LiuNo ratings yet
- Integration Activity 4 2013Document10 pagesIntegration Activity 4 2013Frankie LiuNo ratings yet
- Evals 11 DiureticsDocument8 pagesEvals 11 DiureticsFrankie LiuNo ratings yet
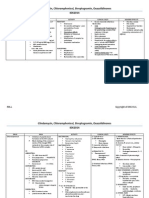
- Clindamycin, Chloramphenicol, Streptogramin, Oxazolidinones IDK2014Document4 pagesClindamycin, Chloramphenicol, Streptogramin, Oxazolidinones IDK2014Frankie LiuNo ratings yet
- Output 4Document10 pagesOutput 4Frankie LiuNo ratings yet
- Patho Prax DemoDocument37 pagesPatho Prax DemoFrankie LiuNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Healthcare Domain Course MaterialDocument131 pagesHealthcare Domain Course Materialdovesnest_in100% (3)
- Epifisiolisis 4Document66 pagesEpifisiolisis 4Eliana Umba PeñaNo ratings yet
- Career GoalsDocument3 pagesCareer GoalsAnalisa PodgorskiNo ratings yet
- Orientee Evaluation SheetDocument5 pagesOrientee Evaluation Sheetjommelryanclumibao2048No ratings yet
- Chlorpromazine Drug StudyDocument3 pagesChlorpromazine Drug StudyPeyjey100% (1)
- Critical Appraisal of Harm/Association StudiesDocument26 pagesCritical Appraisal of Harm/Association Studiesmirfanjee89No ratings yet
- Guideline Chronic Stable AnginaDocument21 pagesGuideline Chronic Stable AnginarinadillaNo ratings yet
- NuplazidDocument14 pagesNuplazidRaquelNo ratings yet
- Lung Center v. Quezon CityDocument8 pagesLung Center v. Quezon CityMassabielleNo ratings yet
- 09 Lec NotesDocument9 pages09 Lec NotesEvilasio CostaNo ratings yet
- Jewish Standard, September 28, 2018Document52 pagesJewish Standard, September 28, 2018New Jersey Jewish StandardNo ratings yet
- The Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Document11 pagesThe Health Anxiety Inventory - Development and Validation of Scales For The Measurement of Health Anxiety and Hypochondriasis 2002Catalina NedelciuNo ratings yet
- Marinella Justine L. Payawal: ObjectiveDocument2 pagesMarinella Justine L. Payawal: Objectiveapi-401676443No ratings yet
- Prosthodontics Inroductory Lecture (Lecture #0)Document5 pagesProsthodontics Inroductory Lecture (Lecture #0)JustDen09No ratings yet
- Dental Assistant Practice ExamDocument5 pagesDental Assistant Practice ExamFaye Nervanna Alecha Alferez100% (8)
- Vaginismo EmdrDocument5 pagesVaginismo EmdrGisela Lucía BachNo ratings yet
- Clinical Examination of A Case of ParaplegiaDocument27 pagesClinical Examination of A Case of Paraplegiaswathi bs0% (2)
- Claim Form Word FrontDocument1 pageClaim Form Word FrontRovic MongcalNo ratings yet
- Dental Management of Patient With Leukemia PedoDocument26 pagesDental Management of Patient With Leukemia PedoFourthMolar.comNo ratings yet
- July 2012 Nle Tips-Chn and CDDocument7 pagesJuly 2012 Nle Tips-Chn and CDJerome Asuncion67% (3)
- Chapter 4 Powerpoint: AnxietyDocument45 pagesChapter 4 Powerpoint: AnxietyJoshNo ratings yet
- Hospital and Laboratory Services (Franz's 1st Update)Document7 pagesHospital and Laboratory Services (Franz's 1st Update)Franz CantaraNo ratings yet
- Toy Cleaning Policy GuideDocument11 pagesToy Cleaning Policy GuideVera IndrawatiNo ratings yet
- Female Male Pelvis Anatomy Radiology Student Version PDFDocument66 pagesFemale Male Pelvis Anatomy Radiology Student Version PDFVictoria MaidmanNo ratings yet
- Electrical SafetyDocument68 pagesElectrical SafetyRafaelAndresOspinoNo ratings yet
- Final Human Bone Morphogenetic ProteinDocument23 pagesFinal Human Bone Morphogenetic Proteinbiologicscorp100% (1)
- Dental Assisting Sample TestDocument26 pagesDental Assisting Sample TestFaye Nervanna Alecha Alferez100% (1)
- HyperbilirubinemiaDocument10 pagesHyperbilirubinemiachiboogs456100% (1)
- Consolidated List of Empanelled HospitalsDocument37 pagesConsolidated List of Empanelled HospitalsAdityaKumarNo ratings yet
- Eric Reichenbach Capstone PaperDocument11 pagesEric Reichenbach Capstone Paperapi-318762550No ratings yet