Professional Documents
Culture Documents
State of The Art and Science of Endodontics
Uploaded by
Emeka V. ObiOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
State of The Art and Science of Endodontics
Uploaded by
Emeka V. ObiCopyright:
Available Formats
State of the art and science of endodontics SHAHROKH SHABAHANG and MEMBERS OF AND CONSULTANTS TO THE AMERICAN ASSOCIATION
OF ENDODONTICS RESEARCH AND SCIENTIFIC AFFAIRS COMMITTEE J Am Dent Assoc 2005;136;41-52
The following resources related to this article are available online at jada.ada.org ( this information is current as of July 28, 2008 ):
Updated information and services including high-resolution figures, can be found in the online version of this article at:
http://jada.ada.org/cgi/content/full/136/1/41
Downloaded from jada.ada.org on July 28, 2008
This article appears in the following subject collections: Endodontics http://jada.ada.org/cgi/collection/endodontics Information about obtaining reprints of this article or about permission to reproduce this article in whole or in part can be found at:
http://www.ada.org/prof/resources/pubs/jada/permissions.asp
2008 American Dental Association. The sponsor and its products are not endorsed by the ADA.
ABSTRACT
Background. Advances in the art and science of endodontics have facilitated better underA D A J standing of disease pro cesses and have led to development of treatment modalities aimed to N C restore health to the pulp A U I N G E D U 1 RT and periradicular tissues. I CLE This article presents a summary of both basic and clinical breakthroughs in endodontics. Results. The author indicates that, on the basis of the reviewed literature, pulp and periradicular diseases are primarily microbial. Basic research has led to development of methodologies that have allowed for specific and accurate identification of pathogens that are likely to cause persistent infections. Close examination of clinical data shows that meticulous dbridement of the infected root canal system will result in a high probability of successful treatment outcome. Progress in visualization, mechanical and chemical disinfection, and biological seal of portals of entry will improve quality of care further. Conclusions and Clinical Implications. A better understanding of the pathogenesis of pulp and periradicular diseases, inflammation and healing, as well as of pain pathways, will improve patient care and result in preservation of natural tissues. Key Words. Endodontics; endodontic technology; basic endodontic research.
A
T
COVER STORY
State of the art and science of endodontics
SHAHROKH SHABAHANG, D.D.S., M.S., Ph.D.; AND MEMBERS OF AND CONSULTANTS TO THE AMERICAN ASSOCIATION OF ENDODONTICS RESEARCH AND SCIENTIFIC AFFAIRS COMMITTEE
IO N
CON
Downloaded from jada.ada.org on July 28, 2008
he past 10 years have witnessed significant changes in the art and science of endodontics. The advances in the science of this specialty have allowed for better understanding of endodontic disease processes and have led to development of treatment modalities aimed at restoring health to the pulp and periradicular tissues. Technological discoveries in instruments and materials have made it possible to achieve treatment objectives that once were considered unattainable. This article reviews the advances in endodonA better tics during the past decade, focusing on understanding both basic and clinical research. of the BASIC RESEARCH pathogenesis of pulp and The microbial nature of endodontic disease. While the mechanical and periradicular manual challenges of root canal dbridediseases will ment and obturation remain, it has improve become increasingly clear that the patient care largest proportion of endodontic disease, and result in both pulpal and periradicular, is due to preservation of the presence of microorganisms. Therefore, treatment success is related very natural tissues. closely to the ability to remove these irritants and to prevent reinfection. The polymicrobial nature of endodontic infections contributes to the increased overall bacterial irritation that is associated with the development of certain virulent bacterial combinations.1-3 The presence of certain microorganisms, such as members of the black-pigmented gram-negative bacteria, in root canals of teeth with necrotic pulp has been associated with increased clinical symptoms.4-6 Development of DNA- and RNA-based microbiological techniques has allowed researchers in endodontics to
identify new species of bacteria7,8 and to develop a more elaborate description of the microbial diversity in root canal infections.9,10 Owing to increased sensitivity and the ability to detect uncultivable microorganisms, researchers identified several fastidious or uncultivable microorganisms in root canal infections, using techniques based on the polymerase chain reaction to amplify the bacterial 16S rRNA gene.8 Researchers cultured grampositive bacteria, particularly Entero41
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
coccus faecalis, from the root canals of teeth with tion. Hard-tissue dissolution is not a characterpersistent periradicular lesions.11-13 Furthermore, istic of pulpal inflammation. The periradicular other researchers cultured fungimostly lesion has proven to be a productive model for the belonging to the genus Candidafrom nearly study of inflammatory resorption.26,27 Clinicians 7 percent of retreatment cases that have culnow have detailed descriptions of the inflammativable microorganisms.14 It is not yet clear tory cascade of cytokines released by bacterial whether these microorganisms cause the treattoxins from macrophages and neutrophils, and ment failure or are favored by the environment of the recognition of a group of these cytokines previously treated root canals. (interleukin-1 alpha, interleukin-2 beta, transThe endodontic literature has devoted much forming growth factor-1 alpha, transforming attention to the question of whether microorgangrowth factor-2 beta) as the osteoclast-activating isms are present within periradicular lesions. factor is an important advance. Techniques using in situ staining methods have For most patients, pain is the most obvious and revealed the presence of bacteria, mainly important characteristic of inflammatory disease, belonging to the genus Actinomyces, in some and especially so when it is within the tooth. therapy-resistant cases.15 Using During inflammation, intrapulpal careful sampling techniques, nerves sprout and gather increased Inflammation and researchers have detected bacteria16 amounts of neuropeptides20 and 17,18 or bacterial DNA in periradicular release transmitters in response to infection of the lesions. More recently, researchers stimulation by cytokines.21 A- fiber periradicular tissues have linked symptomatic periradicterminals, in dentin responding to are an extension of ular lesions to an increased prevahydrodynamic stimuli, and C fibers, the processes in lence of human cytomegalovirus and in pulp responding to inflammatory the pulp but are not Epstein-Barr virus.19 mediators, appear to have differenidentical to them. Inflammation of the pulp. tial roles in pulpitis.28 A relationInflammation of the dental pulp is a ship between symptoms and inflambasic biological response that takes matory molecules has been place in a unique low-compliance environment demonstrated in all studies reporting the signifiand is the result, at least initially, of bacterial cance of substance P.29-31 Inflammation and regentoxins acting well in advance of any direct microeration are closely related. The repair potential of bial invasion. The initial innate component of the the dental pulp is well-known, and recent work response is largely vascular and due to the using growth factors suggests that modulation of release, initiated by cytokines and mediators, of these proteins will be of great value in extending neuropeptides20,21 from the multitude of pulpal the range of pulpal repair procedures.32,33 22 nerves via axon reflexes. A three-dimensional CLINICAL RESEARCH study has revealed widespread anastomoses and loops23 that help limit the potentially damaging Treatment outcomes. The most recent data sequelae of inflammation. In this regard, examiindicate that about 15.8 million primary endonation of a microvascular study24 showed clearly dontic procedures were performed in the United that mechanisms in the capillary bed limit the States in 1999.34 Maintenance of the natural dendangers of increasing tissue fluid pressure such tition, aided by endodontic, periodontal and that capillary collapse occurs only at a late stage restorative procedures, is the preferred choice of in untreated inflammation. Researchers also have patients and remains a predictable treatment mapped out the immunological component of the plan. From the patients perspective, retention of tissue response in detail,25 starting with antigena tooth in a functional and esthetic condition may presenting cells that greet the penetrating irribe considered a favorable treatment outcome. On tants as they reach the odontoblastic layer and the other hand, endodontists use more rigorous culminating in nonspecific and specific responses standards to assess treatment outcomes. Sucby phagocytes and lymphocytes, respectively. cessful treatment to the specialist generally is Inflammation and infection of the periradicular signified by clinical and radiographic absence of tissues are an extension of the processes in the disease. Researchers have reported outcome data pulp but are not identical to them. What practiin the endodontic literature as complete healing, tioners detect most often clinically is bone resorpincomplete healing or an absence of healing. Com42 JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
Downloaded from jada.ada.org on July 28, 2008
R E S E A R C H
plete restoration to health may be expected in 80 percent35,36 to more than 95 percent37 of cases, depending on the observation period. It is important to note that while signs of initiated, but incomplete, healing may be visible in early followup periods, complete resolution of preoperative radiolucent lesions may require up to four years of healing time.38 Overall, the criteria used for reporting endodontic treatment outcomes are different from and more rigorous than those used to report the survival rates of implants. Evidence-based endodontics. Clinical decision making is becoming more complex today and requires information from many sources: primary data and patient preferences, the clinicians own clinical and personal experiences, external rules and constraints, and scientific evidence. There also has been an explosive increase in the amount and quality of laboratory and clinical evidence. Fortunately, mechanisms such as systematic reviews are emerging that will help us acquire the best, most compelling and most current evidence that addresses defined clinical questions. In 1999, the American Association of Endodontists (AAE) Board of Directors elected to use an evidence-based approach to its decision making and embrace lifelong learning as an essential element in the practice of the highest standards of endodontics. Trained AAE members, active in education and research, conducted systematic reviews in selected topics that were reported at the 2002 AAE Annual Session in Chicago. The organization established an Evidence-based Endodontics Standing Committee to consider action on the following recommendations: dconstruction of a critically approved database of identified articles; ddevelopment of an electronic journal from the database; dcontribution to other databases such as the Cochrane Collaboration; dcontinued training of reviewers to conduct systematic reviews on additional clinical questions; dcreation of a standardized report-writing format; drevision of the standards of the American Dental Association Commission on Dental Accreditation to include instruction in conducting systematic reviews.
CLINICAL PRACTICE
Diagnosis. Accurate and efficient diagnosis is the cornerstone of endodontic therapy. Experi-
enced clinicians long have recognized that the patients chief complaint and history of illness are the first, and arguably the most, important pieces of the diagnostic puzzle. Some investigators view history of moderate-to-severe pain as a good indicator of irreversible pulpal pathosis.39 Nonetheless, clinical signs and symptoms alone are unreliable predictors of pulp and periradicular diseases.40,41 Thermal (cold and heat) and electrical pulp testing (EPT) are simple tests but are not completely reliable. Heat as a pulp test has a relatively high sensitivity but is the least accurate overall of the three common pulp tests owing to low specificity.42 Cold testing with tetraflouroethane, ethyl chloride or carbon dioxide (CO2) snow is relatively reliable and generally more accurate than heat. Cold testing is presumed to be more reliable than EPT in teeth with incomplete root formation. Since thermal tests are not 100 percent accurate, EPT is especially useful for confirming a questionable pulpal diagnosis. A major limitation of thermal testing and EPT is that these tests measure only pulpal nerve response, not pulpal blood flow. Since the true measure of pulp vitality is blood flow, laser Doppler flowmetry (LDF) and pulse oximetry devices have been adapted for experimental use in assessing pulp vitality.43-46 These devices seem particularly well-suited for evaluating the vitality of traumatized teeth and for evaluating teeth in areas that may require orthognathic surgery.47 Some investigators have attempted to identify biological factors that may determine the health status of the pulp tissue more accurately.48,49 Identification of the 20,000 to 25,000 genes of the human genome has paved the way for association of specific genes with known pathological findings. Microarray technology has enabled researchers to identify and study a large array of genes and proteins that are affected during disease formation and healing.50,51 Canal instrumentation. The goals of dbridement are to remove irritants from the root canal system and to create a three-dimensional shape that can be obturated.52 Nickel titanium (NiTi) files have become a mainstay in most endodontic procedures. Thanks to this metal, practitioners can use rotary instruments effectively in curved canals. Many file designs and shapes can be used for dbridement. Varying the taper of the instrument leads to a more efficient preparation of the root canal space. Many of these types of files fea43
Downloaded from jada.ada.org on July 28, 2008
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
ture a U-shaped groove and a radial land that the plasticized mass. Use of solid-core carriers helps prevent perforations and instrument such as Thermafil (Dentsply Tulsa Dental, locking and separation. They also usually have a Tulsa, Okla.) is another accepted method of noncutting tip that helps to decrease transportaobturating root canals. By this method, a central tion of the canal space. carrier coated with alpha-phase gutta-percha is While it can reduce the bacterial count signifiwarmed and plasticized in a special oven and cantly, mechanical dbridement does not disinfect inserted to the appropriate depth in the the root canal system completely.53 Thus, a root prepared canal. canal irrigant is needed to aid in the dbridement An apical third obturator acts as a terminal of the canals. Sodium hypochlorite (NaOCl) is the plug at the apical portal of exit. The plug can be most commonly used root canal irrigant. Howmade up of dentin chips formed from the cleaned, ever, NaOCl has some major shortshaped and disinfected canal walls. comings, including its inability to Not only does the plug prevent remove the smear layer54,55 and to overfilling, but also dentin chips The loss of a kill all bacteria present in infected can stimulate the formation of a provisional coronal root canals.12,56,57 Recently, a mixcementumlike cap over the apex.61 access restoration ture of a tetracycline isomer, an Calcium hydroxide62 and mineral most likely results in acid and a detergent known as trioxide aggregate (MTA)63 also can MTAD has been introduced as a be packed as an apical plug. The a compromised root final rinse for disinfection of the remainder of the canal space can be canal seal sometime root canal system. This irrigant is during the first month filled using sealer and a guttaable to remove the smear layer percha gun such as Obtura II of exposure to oral safely,55 and it is a more effective (Obtura Spartan, Fenton, Mo.). contaminants. disinfectant than NaOCl even The lack of a coronal seal is an against resistant bacteria such as important factor in the developE. faecalis.58,59 ment of periradicular lesions folObturation: new delivery systems and lowing root canal therapy.64 Thereimportance of coronal restoration. fore, it is important to prevent coronal leakage Researchers have attributed failure of root canal after completion of root canal therapy. therapy largely to incomplete obturation of the A number of studies have investigated the loss root canal system.60 After proper cleaning, of the provisional restoration to determine how shaping and disinfection of the root canal system, long it takes for coronal leakage to adversely proper filling of the canal is necessary to prevent affect the root canal seal.65-68 In one study, leakage reinfection. There are two basic methods of root occurred in as little as three days time.65 By day canal obturation, with a number of permutations 19 in another study, more than 50 percent of the to these techniques. The lateral condensation root canals were completely contaminated,66 and technique requires lateral compaction of cold by day 30 in a third study, all canals without a gutta-percha points to fill the space. Warm guttacoronal seal were contaminated.68 While the prespercha techniques, also called vertical comence of a temporary restoration may retard this paction techniques, use warm gutta-percha that process, this protection is short-lasting and a subis made plastic and compacted apically. Both stantial change occurs between 28 and 90 days techniques require addition of a cementlike sealer after placement of a temporary restoration.67 that adheres to the dentin walls and fills any The loss of a provisional coronal access restoraspace not obliterated by the gutta-percha. Proption most likely results in a compromised root erly prepared canalscleaned, disinfected and canal seal sometime during the first month of tapered in shapealso should be cleared of the exposure to oral contaminants. Should there be smear layer. This can be achieved by using a coman extended period between the completion of bination of ethylene diamine tetra-acetic acid and endodontic therapy and definitive restorative or NaOCl or MTAD. prosthodontic care, then a definitive restoration Variations of the techniques described previshould be placed in the most coronal portion of ously use newer devices, which are equipped the access opening. with a heated spreader/plugger that warms the Adjuncts. Operating microscopes. Perhaps no gutta-percha and acts as a plugger to compact area of endodontic practice has met with more
44 JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
Downloaded from jada.ada.org on July 28, 2008
R E S E A R C H
excitement and controversy in the past decade than the introduction of the operating microscope (OM) to clinical practice. In less than 10 years, the OM has progressed from a novelty item to a required training standard for specialty education in endodontics. The OM is used most commonly to assist in retrieving separated instruments, locating and negotiating calcified canals, and providing surgical root canal treatment.69 Proponents of OMs feel strongly that they allow for more efficient and safe treatment of teeth that otherwise might be untreatable or treatable only with great difficulty. There is some evidence that the use of OMs in combination with operator skill, prudent case selection, and other current technology and materials may lead to improved surgical treatment outcomes70 and the location of additional canals.71,72 Endoscopes, orascopes and magnifying loupes with or without a supplemental light source also can be employed to enhance visualization of the operative field.73,74 Ultrasonic devices. Ultrasonic devices have become essential tools for assisting in the removal of posts and separated instruments, as well as root-end preparation during surgical treatment of root canals.75 Since heat is a byproduct of the energy generated by ultrasonic instruments, it is important to use a water coolant spray and to operate at the lowest setting possible consistent with the task (root-end preparation, for example, is a delicate procedure and requires a lower setting than do post removal applications). Many specially designed ultrasonic tips are available and suitable for specific situations such as preparing root ends, removing posts, removing instrument fragments and searching for calcified canals. Ultrasonic tips specially designed for rootend preparation allow for conservative and precise preparation of the root end during apical surgery. Electronic apex locators. The task of determining canal length has moved into a new and more precise era with the rapid evolution of electronic devices that measure the length of the root canal. The first- and second-generation apex locators were more difficult to use and more prone to erroneous readings than are the third-generation devices now available. Research and clinical experience support the claim that apex locators can assist accurately in determining canal length in the majority of cases.76-78 Apex locators also can be used to detect
perforations and root fractures. The use of electronic apex locators is contraindicated in patients with cardiac pacemakers, although the actual risk to these patients is uncertain.79 Lasers. Lasers have various applications in endodontics such as measuring pulp vitality,80 treating dentinal hypersensitivity,81 preparing and disinfecting root canals,82,83 and performing apical surgery.84 Reports about these applications are conflicting, owing to the use of different types of lasers, energy levels and specimens used. LDF has the most promising application in endodontics. LDF was developed to assess blood flow in microvascular systems.85 The reliability of conventional pulp tests can vary in newly erupted and traumatized teeth, owing to incomplete formation or trauma to the neural pulpal component, respectively. LDF techniques are sensitive and accurate for pulp vitality testing because they reflect vascular rather than nervous responsiveness when compared with other methods.44 LDF is a useful research instrument, but a practical clinical device still is lacking. The neodymium:yttrium-aluminum-garnet (Nd:YAG) laser is the most popular system for cleaning and shaping the root canal system, because the device offers a thin fiber-optic delivery system for entering narrow root canals. Lasers can remove the smear layer and debris; however, it is difficult to clean all root canal walls with these devices, because the linear emission of the laser beam makes it almost impossible to irradiate the lateral canal walls and leaves them rough and uneven. Root canal spaces rarely are straight; more often, they are curved in at least two dimensions. For lasers to be useful in endodontics, it is necessary to improve the fiber tip and the method so that the laser irradiates all areas of root canal walls. Several studies have evaluated the sterilization of root canal systems by means of CO286 and Nd:YAG lasers.87 Although lasers used at high power have a bactericidal effect, that effect is dependent on each laser. Furthermore, using lasers to disinfect root canals is problematic, since it can inflict thermal injury on periodontal tissues. Despite lasers approval for dental procedures by the U.S. Food and Drug Administration, more research is required to develop lasers for use in endodontics and to compare their efficacy with that of present treatment modalities.
Downloaded from jada.ada.org on July 28, 2008
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
45
R E S E A R C H
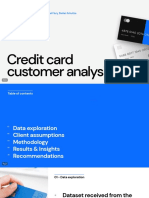
Figure 1. Nonsurgical retreatment allows for threedimensional dbridement and obturation of the root canal system.
SPECIAL CASES
Nonsurgical retreatment (indications versus surgery). Despite the availability of advanced technological tools and better understanding of the biology of pulp and periradicular diseases, clinicians often need to address posttreatment endodontic disease.88 Before commencing with any treatment, clinicians must consider all interdisciplinary treatment options in terms of time, expense, prognosis and patient satisfaction. If the choice is endodontics, then the goal of nonsurgical retreatment is to remove materials from the root canal space and to address any deficiencies or repair defects that are pathological or iatrogenic in origin.89 Many significant advantages result when endodontically failing teeth are re-entered nonsurgically. Endodontic access provides the opportunity to evaluate teeth for coronal leakage, fractures and missed canalsand importantly, after disassembly procedures, these root canal systems can be three-dimensionally cleaned, shaped and obturated (Figure 1).90 Advancements in the field of nonsurgical endodontic retreatment are related directly to the introduction of the dental OM, ultrasonic technology and related instruments, NiTi rotary shaping files and MTA.91 Nonsurgical retreatment of failed cases has a similar success rate to that of initial conventional treatment if the cause of failure is identified and corrected.92 Perforation repairs. Historically, the occurrence of perforations during root canal treatment
46
has reduced the long-term prognosis of the affected tooth significantly. The poor prognosis of perforations is mostly due to bacterial leakage or the lack of biocompatibility of the repair materials used.93 The important steps in the management of a furcal perforation are immediate treatment, adequate isolation, dbridement and sealing of the defect.94 Discovery of new materials such as MTA95,96 has significantly improved the prognosis for what once were considered hopeless teeth.97 Trauma and management of open apexes. Traumatic injuries in young patients present a special challenge during endodontic treatment in terms of diagnosis and treatment planning, as well as of managing the open apex. Whenever possible, the goal should be preservation of pulp vitality to allow continued development along the entire root length.98 MTA has the most desirable properties for this purpose99 because it provides a good seal,100 is biocompatible101 and induces hard-tissue formation.102 If the pulp is necrotic, the treatment of choice is root canal therapy.103 However, in an immature tooth, completion of root canal therapy must be delayed until root-end closure has been completed.104 Long-term calcium hydroxide therapy no longer is the treatment of choice because of the variability of its treatment outcomes and its adverse effects on dentin.105 Researchers have advocated placement of an artificial barrier as an alternative to long-term apexification procedures.62,106,107 More recently, MTA has been shown to induce hard-tissue formation more predictably than calcium hydroxide (Figure 2), while bioactive materials such as bone morphogenetic proteins have demonstrated no added advantage over calcium hydroxide.63 Evaluation of healing of intra-alveolar root fractures in patients between the ages of seven and 17 years suggests that 77 percent of these cases heal by means of development of a hardtissue fragment, development of periodontal ligament or a combination of the two.108 Pulp vitality, degree of tooth development, presence or absence of response of the pulp to stimuli, type of injury, amount of diastasis between the fragments and efforts to reposition the displaced fragments have an influence on healing.108 However, the efficacy of long-term splinting is questionable.108 To prioritize treatment of traumatic injuries, treatment delivery has been divided into three groups109: acute (treatment rendered within a few
Downloaded from jada.ada.org on July 28, 2008
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
hours), subacute (treatment rendered within the first 24 hours) and delayed (treatment rendered after the first 24 hours). A survey of the available literature suggests the following recommendations: dcrown and crown/root fracturessubacute or delayed treatment; droot fracturesacute or subacute treatment; dconcussion and subluxationsubacute treatment; dextrusion and lateral luxationacute or subacute treatment; dintrusionsubacute treatment; davulsionacute treatment if the tooth is not replanted at the time of injury, subacute treatment otherwise; dprimary tooth injurysubacute treatment, unless the primary tooth is displaced into the follicle of the permanent tooth or occlusal problems are present, in which cases acute treatment is necessary. Surgical root canal therapy. Endodontic surgery is not oral surgery in the traditional sense. Rather, it actually is endodontic therapy performed through a surgical flap. The main purpose of performing periradicular surgery is to remove a portion of a root with undbrided canal space or to seal the canal when a complete seal cannot be accomplished through a coronal approach. With recent improvements in surgical instruments, materials and techniques, endodontic surgery can provide a second chance to retain a tooth that otherwise would be extracted. Endodontic surgery may be necessary to address anatomical complexities and procedural complications associated with difficult nonsurgical cases.110-113 The OM is the latest addition to this armamentarium, providing up to 32 magnification of the surgical field.114,115 The quantity and quality of light in the working field is as important as magnification. The coaxial lighting and improved optics of an OM provide better distinction between tooth and bone. Identifying minute canal openings, incipient fracture lines and other important anatomical findings becomes routine with the OM. For example, an isthmus frequently runs between two canals in the mesiobuccal root of the maxillary first molar.116,117 These small communications contain pulp tissue remnants and should be included in root-end cavity preparations and fillings during endodontic surgery.118 The magnification and illumination afforded by the OM facilitates identification of
A Downloaded from jada.ada.org on July 28, 2008
B
Figure 2. A. Radiograph demonstrating a mandibular premolar with an incompletely developed root and an open apex. B. Radiograph demonstrating formation of a hardtissue barrier at the root end of the premolar after treatment with mineral trioxide aggregate as an apical plug.
these ramifications, allowing them to be prepared and filled with the main canals (Figure 3). Enhanced magnification necessitates miniaturization of endodontic surgical instruments. Microscalpels, piezoelectric ultrasonic handpieces, surgical micromirrors and microsurgical irrigators, together with miniature carriers, condensers and pluggers, have been developed to accommodate the high level of magnification used routinely in endodontic surgical procedures. The miniaturized instruments allow more precise performance of surgical procedures. For instance, the root-end preparation is aligned parallel to the long axis of the root using specially designed ultrasonic tips to a depth of 3 mm.119 A variety of root-end filling materials can be used, which include Super EBA (Harry J. Bosworth, Skokie, Ill.), intermediate restorative material, dentin bonding agents and, most recently, MTA.118,120,121 The materials should be biocompat47
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
Figure 3. Clinical photograph demonstrating an isthmus connecting the two canals in the mesial root of a mandibular first molar.
Figure 4. Photomicrograph (original magnification 50, hemotoxylin and eosin stain) demonstrating a complete cementum layer over a resected root end filled with mineral trioxide aggregate.
ible, provide a hermetic seal and, ideally, stimulate hard-tissue growth. MTA provides a superior apical seal compared with other root-end filling materials and is not adversely affected by blood contamination. In several studies, histologic sections demonstrate the regeneration of new cementum over the MTA root-end filling (Figure 4), a phenomenon that is not seen with other commonly used root-end filling materials. Clinical controversy: the smear layer. Studies have shown that current methods of cleaning and shaping root canals produce a smear layer that covers the instrumented walls.54,122-125
48
The smear layer contains inorganic and organic substances that include fragments of odontoblastic processes, microorganisms and necrotic materials. Proponents of smear layer removal claim that the presence of a smear layer can inhibit or significantly delay penetration of antimicrobial agents such as intracanal irrigants and medications into the dentinal tubules.126,127 Furthermore, removal of the smear layer may significantly improve adhesion of obturation materials to the canal walls128-132 and reduce microleakage.132-137 While some investigators have reported that the removal of the smear layer does not have any significant effect on microleakage of root canals,138-140 the opponents of smear layer removal have shown an increased level of leakage through the obturated root canals141 with a 10- to 80micrometer depth of penetration.142-146 Despite controversy regarding the effect of the smear layer on the quality of instrumentation and obturation, it should be noted that the smear layer itself may be infected and may protect the bacteria already present in the dentinal tubules.54,147,148 Because of these concerns, it may be prudent to remove the initially created smear layer from infected root canals and allow penetration of intracanal medications into the dentinal tubules of these teeth. After disinfection of the root canal system, the smear layer can be recreated. Chemical, mechanical and laser means can be used to remove the smear layer. Management of pain, infection and anxiety. Considerable advances have occurred in the management of pain, infection and anxiety in the endodontic patient. Pain. Survey studies indicate that only about 40 percent of patients report pain after nonsurgical root canal therapy, with about 20 to 25 percent reporting moderate-to-severe pain.149 Thus, the clinician should tailor pain management strategies to each patient. A survey of endodontic clinical trials indicated that the presence of preoperative pain or a positive response to percussion is a consistent predictor of patients most likely to report postendodontic pain.150 A systematic review of nonsteroidal anti-inflammatory drugs used to treat pain in endodontic patients reported good analgesic responses in patients treated with either 100 milligrams of flurbiprofen or the combination of flurbiprofen with 100 mg of tramadol.151 In the classic case of the difficult-to-anesthetize mandibular molar, several studies have demon-
Downloaded from jada.ada.org on July 28, 2008
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
strated that intraosseous anesthetics are effective for enhancing the incomplete anesthesia that occurs after inferior alveolar nerve block injection.152,153 Infection. Considerable progress has been made with respect to the use of antibiotics in endodontic patients. Susceptibility testing studies have indicated that 80 to 95 percent of cultivable endodontic microorganisms remain sensitive to penicillin, supporting the selection of penicillin as an antibiotic of first choice when indicated.154,155 Clindamycin is a good alternative for patients who are unable to take penicillin, since approximately 87 to 100 percent of cultivable endodontic microorganisms are sensitive to this antibiotic.154,155 Although antibiotics are effective for treating endodontic infections, they appear to have little effect on reducing pain.156 In addition, antibiotics have no effect when prescribed to treat pain due to irreversible pulpitis.157 Anxiety. Researchers have evaluated several approaches for treating anxiety associated with endodontic care. In general, both behavioral and pharmacological methods have proven to be effective. Oral triazolam (0.25 mg) may be superior to oral diazepam (5 mg) for reducing anxiety associated with endodontic treatment.158
CONCLUSIONS AND FUTURE DIRECTIONS
This work was made possible by the contributions of the members of and consultants to the American Association of Endodontics Research and Scientific Affairs Committee who contributed to this report: Drs. Leif K. Bakland, Mario DAddario, Mohamed F. Fayad, Ashraf Fouad, Charles J. Goodacre, Kenneth M. Hargreave, G.R. Holland, John I. Ingle, Bradford R. Johnson, Sergio Kuttler, Jeffrey Lilly, Robert J. Loushine, Andre Mickel, Carl W. Newton, Ilan Rotstein, Clifford J. Ruddle, Charles L. Steffel and Mahmoud Torabinejad. 1. Baumgartner JC, Falkler WA Jr, Beckerman T. Experimentally induced infection by oral anaerobic microorganisms in a mouse model. Oral Microbiol Immunol 1992;7(4):253-6. 2. Sundqvist G. Associations between microbial species in dental root canal infections. Oral Microbiol Immunol 1992;7(5):257-62. 3. Siqueira JF Jr, Magalhaes FA, Lima KC, de Uzeda M. Pathogenicity of facultative and obligate anaerobic bacteria in monoculture and combined with either Prevotella intermedia or Prevotella nigrescens. Oral Microbiol Immunol 1998;13(6):368-72. 4. Griffee MB, Patterson SS, Miller CH, Kafrawy AH, Newton CW. The relationship of Bacteroides melaninogenicus to symptoms associated with pulpal necrosis. Oral Surg Oral Med Oral Pathol 1980;50(5):457-61. 5. Yoshida M, Fukushima H, Yamamoto K, Ogawa K, Toda T., Sagawa H. Correlation between clinical symptoms and microorganisms isolated from root canals of teeth with periapical pathosis. J Endod 1987;13(1): 24-8. 6. Sundqvist G, Johansson E, Sjgren U. Prevalence of blackpigmented Bacteroides species in root canal infections. J Endod 1989;15(1):13-9. 7. Gharbia SE, Haapasalo M, Shah HN, et al. Characterization of Prevotella intermedia and Prevotella nigrescens isolates from periodontic and endodontic infections. J Periodontol 1994;65(1):56-61. 8. Baumgartner JC, Bae KS, Xia T, Whitt J, David LL. Sodium dodecyl sulfate-polyacrylamide gel electrophoresis and polymerase chain reaction for differentiation of Prevotella intermedia and Prevotella nigrescens. J Endod 1999;25(5):324-8. 9. Dymock D, Weightman AJ, Scully C, Wade WG. Molecular analysis of microflora associated with dentoalveolar abscesses. J Clin Microbiol 1996;34(3):537-42. 10. Munson MA, Pitt-Ford T, Chong B, Weightman A, Wade WG. Molecular and cultural analysis of the microflora associated with endodontic infections [published correction appears in J Dent Res 2003;82(1):69 and in J Dent Res 2003;82(3): 247]. J Dent Res 2002;81(11):761-6. 11. Molander A, Reit C, Dahlen G, Kvist T. Microbiological status of root-filled teeth with apical periodontitis. Int Endod J 1998;31(1):1-7. 12. Sundqvist G, Figdor D, Persson S, Sjgren U. Microbiologic analysis of teeth with failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85(1):86-93. 13. Hancock HH 3rd, Sigurdsson A, Trope M, Moiseiwitsch J. Bacteria isolated after unsuccessful endodontic treatment in a North American population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91(5):579-86. 14. Waltimo TM, Siren EK, Torkko HL, Olsen I, Haapasalo MP. Fungi in therapy-resistant apical periodontitis. Int Endod J 1997;30(2):96-101. 15. Happonen RP. Periapical actinomycosis: a follow-up study of 16 surgically treated cases. Endod Dent Traumatol 1986;2(5):205-9. 16. Sunde PT, Olsen I, Lind PO, Tronstad L. Extraradicular infection: a methodological study. Endod Dent Traumatol 2000;16(2):84-90. 17. Gatti JJ, Dobeck JM, Smith C, White RR, Socransky SS, Skobe Z. Bacteria of asymptomatic periradicular endodontic lesions identified by DNA-DNA hybridization. Endod Dent Traumatol 2000;16(5):197-204. 18. Sunde PT, Tronstad L, Eribe ER, Lind PO, Olsen I. Assessment of periradicular microbiota by DNA-DNA hybridization. Endod Dent Traumatol 2000;16(5):191-6. 19. Sabeti M, Valles Y, Nowzari H, Simon JH, Kermani-Arab V, Slots J. Cytomegalovirus and Epstein-Barr virus DNA transcription in endodontic symptomatic lesions. Oral Microbiol Immunol 2003;18(2): 104-8. 20. Byers MR, Narhi MV. Dental injury models: experimental tools for understanding neuroinflammatory interactions and polymodal nociceptor functions. Crit Rev Oral Biol Med 1999;10:4-39. 21. Goodis HE, Bowles WR, Hargreaves KM. Prostaglandin E2 enhances bradykinin-evoked iCGRP release in bovine dental pulp. J Dent Res 2000;79:1604-7. 22. Olgart L. Neural control of pulpal blood flow. Crit Rev Oral Biol Med 1996;7:159-71.
Downloaded from jada.ada.org on July 28, 2008
The art and science of endodontics have undergone significant advances in the past decade. These changes have resulted in improved treatment outcomes and an opportunity to preserve the natural dentition. These objectives can be achieved with less morbidity and more predictability. The specialty of endodontics is dedicated to the preservation of healthy natural dentition. Compilation of more current clinical data that are based on procedures performed with more advanced techniques will provide a more accurate rate of healing after nonsurgical and surgical endodontic therapy. The future holds the promise of continued growth of the body of research knowledge, and systematic reviews will provide the most valuable thread of evidence connecting the patient, the clinician, the educator, the researcher, the policy-maker, the editor, the benefit purchaser and the benefit provider in the decision-making process. s
Dr. Shabahang is the chair, Research and Scientific Affairs Committee, Loma Linda University, Department of Endodontics, P.O. Box 1057, Loma Linda, Calif. 92354-1057, e-mail sshabahang@ sd.llu.edu. Address reprint requests to Dr. Shabahang.
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
49
R E S E A R C H
23. Takahashi K. Changes in the pulpal vasculature during inflammation. J Endod 1990;16:92-7. 24. Heyeraas KJ, Berggreen E. Interstitial fluid pressure in normal and inflamed pulp. Crit Rev Oral Biol Med 1999;10:328-36. 25. Jontell M, Okiji T, Dahlgren U, Bergenholtz G. Immune defense mechanisms of the dental pulp. Crit Rev Oral Biol Med 1998;9:179-200. 26. Stashenko P, Teles R, DSouza R. Periapical inflammatory responses and their modulation. Crit Rev Oral Biol Med 1998;9: 498-521. 27. Fouad A. Are antibiotics effective for endodontic pain? An evidence-based review. Endod Topics 2002;3:52-66. 28. Narhi M, Jyvasjarvi E, Virtanen A, Huopaniemi T, Ngassapa D, Hirvonen T. Role of intradental A- and C-type nerve fibres in dental pain mechanisms. Proc Fin Dent Soc 1992;88:507-16. 29. Rodd HD, Boissonade FM. Substance P expression in human tooth pulp in relation to caries and pain experience. Eur J Oral Sci 2000;108:467-74. 30. Awawdeh L, Lundy FT, Shaw C, Lamey PJ, Linden GJ, Kennedy JG. Quantitative analysis of substance P, neurokinin A and calcitonin gene-related peptide in pulp tissue from painful and healthy human teeth. Int Endod J 2002;35:30-6. 31. Bowles WR, Withrow JC, Lepinski AM, Hargreaves KM. Tissue levels of immunoreactive substance P are increased in patients with irreversible pulpitis. J Endod 2003;29:265-7. 32. Goldberg M, Six N, Decup F, et al. Application of bioactive molecules in pulp-capping situations. Adv Dent Res 2001;15:91-5. 33. Smith AJ, Murray PE, Sloan AJ, Matthews JB, Zhao S. Transdentinal stimulation of tertiary dentinogenesis. Adv Dent Res 2001;15:51-4. 34. American Dental Association. The 1999 survey of dental services rendered. Chicago: American Dental Association; 2002:16. 35. Friedman S, Lost C, Zarrabian M, Trope M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J Endod 1995;21(7):384-90. 36. Caliskan MK, Sen BH. Endodontic treatment of teeth with apical periodontitis using calcium hydroxide: a long-term study. Endod Dent Traumatol 1996;12(5):215-21. 37. Sjgren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990;16(10): 498-504. 38. rstavik D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int Endod J 1996;29(3):150-5. 39. Bender IB. Pulpal pain diagnosis: a review. J Endod 2000;26(3): 175-9. 40. Hyman JJ, Cohen ME. The predictive value of endodontic diagnostic tests. Oral Surg Oral Med Oral Pathol 1984;58(3):343-6. 41. Michaelson PL, Holland GR. Is pulpitis painful? Int Endod J 2002;35(10):829-32. 42. Petersson K, Soderstrom C, Kiani-Anaraki M, Levy G. Evaluation of the ability of thermal and electrical tests to register pulp vitality. Endod Dent Traumatol 1999;15(3):127-31. 43. Ingolfsson AR, Tronstad L, Hersh EV, Riva CE. Efficacy of laser Doppler flowmetry in determining pulp vitality of human teeth. Endod Dent Traumatol 1994;10(2):83-7. 44. Evans D, Reid J, Strang R, Stirrups D. A comparison of laser Doppler flowmetry with other methods of assessing the vitality of traumatised anterior teeth. Endod Dent Traumatol 1999;15(6):284-90. 45. Schnettler JM, Wallace JA. Pulse oximetry as a diagnostic tool of pulpal vitality. J Endod 1991;17(10):488-90. 46. Roebuck EM, Evans DJ, Stirrups D, Strang R. The effect of wavelength, bandwidth, and probe design and position on assessing the vitality of anterior teeth with laser Doppler flowmetry. Int J Paediatr Dent 2000;10(3):213-20. 47. Aanderud-Larsen K, Brodin P, Aars H, Skjelbred P. Laser Doppler flowmetry in the assessment of tooth vitality after Le Fort I osteotomy. J Craniomaxillofac Surg 1995;23(6):391-5. 48. Hahn CL, Falkler WA Jr, Siegel MA. A study of T and B cells in pulpal pathosis. J Endod 1989;15(1):20-6. 49. Izumi T, Kobayashi I, Okamura K, Sakai H. Immunohistochemical study on the immunocompetent cells of the pulp in human noncarious and carious teeth. Arch Oral Biol 1995;40(7):609-14. 50. Tjderhane L, Pkknen V, Larmas M, Sulkala M, Salo T. DNA microarray analysis of differential MMP expression in healthy and carious tooth pulp tissue (abstract 537). J Dent Res 2003 (serial on CD-ROM). 51. Tsou R, Cole JK, Nathens AB, et al. Analysis of hypertrophic and normal scar gene expression with cDNA microarrays. J Burn Care Rehabil 2000;21(6):541-50.
52. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974;18(2):269-96. 53. Pataky L, Ivanyi I, Grigar A, Fazekas A. Antimicrobial efficacy of various root canal preparation techniques: an in vitro comparative study. J Endod 2002;28(6):603-5. 54. McComb D, Smith DC. A preliminary scanning electron microscopic study of root canals after endodontic procedures. J Endod 1975;1:238-42. 55. Torabinejad M, Khademi AA, Babagoli J, et al. A new solution for the removal of the smear layer. J Endod 2003;29(3):170-5. 56. Sjgren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis [published correction appears in Int Endod J 1998;31(2):148]. Int Endod J 1997;30(5):297-306. 57. Shuping GB, rstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria using nickel-titanium rotary instrumentation and various medications. J Endod 2000;26:751-5. 58. Torabinejad M, Shabahang S, Aprecio R, Kettering JD. The antimicrobial effect of MTAD: an in vitro investigation. J Endod 2003;29(6):400-3. 59. Shabahang S, Torabinejad M. Effect of MTAD on Enterococcus faecalis-contaminated root canals of extracted human teeth. J Endod 2003;29(9):576-9. 60. Ingle JI. The Washington study of success and failure. In: Ingle JI, Bakland LK, eds. Endodontics. 5th ed. Hamilton, Ontario, Canada: BC Decker; 2002:748. 61. Pitts DL, Jones JE, Oswald RJ. A histological comparison of calcium hydroxide plugs and dentin plugs used for the control of guttapercha root canal filling material. J Endod 1984;10(7):283-93. 62. Schumacher JW, Rutledge RE. An alternative to apexification. J Endod 1993;19(10):529-31. 63. Shabahang S, Torabinejad M, Boyne P, Abedi H, McMillan P. A comparative study of root-end induction using osteogenic protein-1, calcium hydroxide, and mineral trioxide aggregate in dogs. J Endod 1999;24(1):1-5. 64. Snider D, Torabinejad M, Tang HM, Bakland LK. Effect of root canal obturation and/or coronal seal on the success of root canal therapy (abstract 50). J Endod 1999;25:294. 65. Swanson K, Madison S. An evaluation of coronal microleakage in endodontically treated teeth: part Itime periods. J Endod 1987;13(2): 56-9. 66. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J Endod 1990;16(12):566-9. 67. Magura ME, Kafrawy AH, Brown CE Jr, Newton CW. Human saliva coronal microleakage in obturated root canals: an in vitro study. J Endod 1991;17(7):324-31. 68. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed obturated root canals. J Endod 1993;19(9):458-61. 69. Mines P, Loushine RJ, West LA, Liewehr FR, Zadinsky JR. Use of the microscope in endodontics: a report based on a questionnaire. J Endod 1999;25(11):755-8. 70. Rubinstein RA, Kim S. Long-term follow-up of cases considered healed one year after apical microsurgery. J Endod 2002;28(5):378-83. 71. Schwarze T, Baethge C, Stecher T, Geurtsen W. Identification of second canals in the mesiobuccal root of maxillary first and second molars using magnifying loupes or an operating microscope. Aust Endod J 2002;28(2):57-60. 72. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod 2002;28(4):324-7. 73. von Arx T, Hunenbart S, Buser D. Endoscope- and video-assisted endodontic surgery. Quintessence Int 2002;33(4):255-9. 74. Bahcall JK, Barss JT. Fiberoptic endoscope usage for intracanal visualization. J Endod 2001;27(2):128-9. 75. von Arx T, Walker WA 3rd. Microsurgical instruments for rootend cavity preparation following apicoectomy: a literature review. Endod Dent Traumatol 2000;16(2):47-62. 76. Fouad AF, Reid LC. Effect of using electronic apex locators on selected endodontic treatment parameters. J Endod 2000;26(6):364-7. 77. Fouad AF, Krell KV, McKendry DJ, Koorbusch GF, Olson RA. Clinical evaluation of five electronic root canal length measuring instruments. J Endod 1990;16(9):446-9. 78. Dunlap CA, Remeikis NA, BeGole EA, Rauschenberger CR. An in vivo evaluation of an electronic apex locator that uses the ratio method in vital and necrotic canals. J Endod 1998;24(1):48-50. 79. Garofalo RR, Ede EN, Dorn SO, Kuttler S. Effect of electronic apex locators on cardiac pacemaker function. J Endod 2002;28(12): 831-3.
Downloaded from jada.ada.org on July 28, 2008
50
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
R E S E A R C H
80. Gazelius B, Olgart L, Edwall B, Edwall L. Non-invasive recording of blood flow in human dental pulp. Endod Dent Traumatol 1986;2(5): 219-21. 81. Fayad MI, Carter JM, Liebow C. Transient effects of low-energy CO2 laser irradiation on dentinal impedance: implications for treatment of hypersensitive teeth. J Endod 1996;22:526-31. 82. Levy G. Cleaning and shaping the root canal with a Nd:YAG laser beam: a comparative study. J Endod 1992;18:123-7. 83. Hardee MW, Miserendino LJ, Kos W, Walia H. Evaluation of the antibacterial effects of intracanal Nd:YAG laser irradiation. J Endod 1994;20:377-80. 84. Bader G, Lejeune S. Prospective study of two retrograde endodontic apical preparations with and without the use of CO2 laser. Endod Dent Traum 1998;14:75-8. 85. Tronstad L. Recent development in endodontic research. Scand J Dent Res 1992;100:52-9. 86. Zakariasen KL, Dederich DN, Tulip J, DeCoste S, Jensen SE, Pickard MA. Bactericidal action of carbon dioxide laser radiation in experimental dental root canals. Can J Microbiol 1986;32:942-6. 87. Ramskold LO, Fong CD, Stromberg T. Thermal effects and antibacterial properties of energy levels required to sterilize stained root canals with an Nd:YAG laser. J Endod 1997;23:96-100. 88. Scianamblo MJ. Endodontic failures: the retreatment of previously endodontically treated teeth. Revue DOdonto Stomatologie 1988;17(5):409-23. 89. Ruddle CJ. Nonsurgical endodontic retreatment. In: Cohen S, Burns RC, eds. Pathways of the pulp. 8th ed. St. Louis: Mosby; 2002:875-929. 90. Machtou P. La cavit daccs. In: Machtou P, Bensoussan D, Hartmann A, Mandel E, eds. Endodontie. Paris: Editions CdP; 1993;125-37. 91. Ruddle CJ. Microendodontic nonsurgical retreatment. Dent Clin North Am 1997;41(3):429-54. 92. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjo B, Engstrom B. Retreatment of endodontic fillings. Scand J Dent Res 1979;87(3):217-24. 93. Arens DE, Torabinejad M. Repair of furcal perforations with mineral trioxide aggregate: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82(1):84-8. 94. Bryan EB, Woollard G, Mitchell WC. Nonsurgical repair of furcal perforations: a literature review. Gen Dent 1999;47(3):274-8. 95. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J Endod 1993; 19(11):541-4. 96. Ford TR, Torabinejad M, McKendry DJ, Hong CU, Kariyawasam SP. Use of mineral trioxide aggregate for repair of furcal perforations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79(6):756-63. 97. Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of root perforations using mineral trioxide aggregate: a long-term study. J Endod 2004;30(2):80-3. 98. Pitt Ford T, Shabahang S. Management of incompletely formed roots. In: Principles of endodontics. 3rd ed. Philadelphia: Saunders; 2001:388-404. 99. Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp-capping material. JADA 1996;127(10):1491-4. 100. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR. Bacterial leakage of mineral trioxide aggregate as a root-end filling material. J Endod 1995;21(3):109-12. 101. Torabinejad M, Hong CU, Pitt Ford TR, Kettering JD. Cytotoxicity of four root end filling materials. J Endod 1995;21(10):489-92. 102. Koh ET, Torabinejad M, Pitt Ford TR, Brady K, McDonald F. Mineral trioxide aggregate stimulates a biological response in human osteoblasts. J Biomed Mater Res 1997;37(3):432-9. 103. Seltzer S. The root apex. In: Seltzer S, Krasner P, eds. Endodontology. 2nd ed. Philadelphia: Lea & Febiger; 1988:1-30. 104. Frank A. Therapy for the divergent pulpless tooth by continued apical formation. JADA 1966;72(1):87-93. 105. Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol 2002;18(3):134-7. 106. Coviello J, Brilliant JD. A preliminary clinical study on the use of tricalcium phosphate as an apical barrier. J Endod 1979;5(1):6-13. 107. Brandell DW, Torabinejad M, Bakland LK, Lessard GM. Demineralized dentin, hydroxylapatite and dentin chips as apical plugs. Endod Dent Traumatol 1986;2(5):210-4. 108. Cvek M, Andreasen JO, Borum MK. Healing of 208 intraalveolar root fractures in patients aged 7-17 years. Dent Traumatol 2001;17: 53-62. 109. Andreasen JO, Andreasen FM, Skeie A, Hjorting-Hansen E,
Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries: a review article. Dent Traumatol 2002;18:116-28. 110. Gutmann JL, Harrison JW. Surgical endodontics. Boston: Blackwell Scientific; 1991. 111. Bellizzi R, Loushine R. A clinical atlas of endodontic surgery. Chicago: Quintessence; 1991. 112. Arens DE, Torabinejad M, Chivian N, Rubinstein R. Practical lessons in endodontic surgery. Chicago: Quintessence; 1998. 113. Kim S. Color atlas of microsurgery in endodontics. Philadelphia: Saunders; 2001. 114. Pecora G, Andreana S. Use of dental operating microscope in endodontic surgery. Oral Surg Oral Med Oral Path 1993;75:751-8. 115. Mounce RE. Surgical operating microscopes in endodontics: the paradigm shift. Gen Dent 1995;43(4):346-9. 116. Weller RN, Niemczyk SP, Kim S. Incidence and position of the canal isthmus: part 1mesiobuccal root of the maxillary first molar. J Endod 1995;21:380-3. 117. Carr G. Ultrasonic root end preparation. Dent Clin of North Am 1997;41(3):541-54. 118. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod 1993;19:591-5. 119. Gilheany PA, Figdor D, Tyas MJ. Apical dentin permeability and microleakage associated with root end resection and retrograde filling. J Endod 1994;20(1):22-6. 120. Dorn SO, Gartner AH. Retrograde filling materials: a retrospective success-failure study of amalgam, EBA, and IRM. J Endod 1990; 16(8):391-3. 121. Rud J, Rud V, Munksgaard EC. Long-term evaluation of retrograde root filling with dentin-bonded resin composite. J Endod 1996; 22:90-3. 122. Moodnik RM, Dorn SO, Feldman MJ, Levey M, Borden BG. Efficacy of biomechanical instrumentation: a scanning electron microscopic study. J Endod 1976;2:261-6. 123. Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopic investigation of the smeared layer on root canal walls. J Endod 1984;10:477-83. 124. Cengiz T, Aktener BO, Piskin B. The effect of dentinal tubule orientation on the removal of smear layer by root canal irrigants: a scanning electron microscopic study. Int Endod J 1990;23:163-71. 125. Pashley DH. Smear layer: overview of structure and function. Proc Finn Dent Soc 1992;88(supplement l):215-24. 126. rstavik D, Haapasalo M. Disinfection by endodontic irrigants and dressings of experimentally infected dentinal tubules. Endod Dent Traumatol 1990;6:142-9. 127. Bystrm A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J 1985;18:35-40. 128. Abramovich A, Goldberg F. The relationship of the root canal sealer to the dentine wall: an in vitro study using the scanning electron microscope. J Br Endod Soc 1976;9(2):81-6. 129. Tidmarsh BG. Acid-cleansed and resin-sealed root canals. J Endod 1978;4:117-21. 130. White R, Goldman M, Lin PS. The influence of the smeared layer upon dentinal tubule penetration by plastic filling materials. J Endod 1984;10:558-62. 131. Gettleman BH, Messer HH, ElDeeb ME. Adhesion of sealer cements to dentin with and without the smear layer. J Endod 1991; 17:15-20. 132. Economides N, Liolios E, Kolokuris I, Beltes P. Long-term evaluation of the influence of smear layer removal on the sealing ability of different sealers. J Endod 1999;25:123-5. 133. Kennedy WA, Walker WA, Gough RW. Smear layer removal effects on apical leakage. J Endod 1986;12:21-7. 134. Cergneux M, Ciucchi B, Dietschi JM, Holz J. The influence of the smear layer on the sealing ability of canal obturation. Int Endod J 1987;20:228-32. 135. Vassiliadis L, Liolios E, Kouvas V, Economides N. Effect of smear layer on coronal microleakage. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;82:315-20. 136. Taylor JK, Jeansonne BG, Lemon RR. Coronal leakage: effects of smear layer, obturation technique, and sealer. J Endod 1997;23:508-12. 137. Karagz-Kkay I, Bayirli G. An apical leakage study in the presence and absence of the smear layer. Int Endod J 1994;27:87-93. 138. Evans JT, Simon JH. Evaluation of the apical seal produced by injected thermoplasticized gutta-percha in the absence of smear layer and root canal sealer. J Endod 1986;12:100-7. 139. Chailertvanitkul P, Saunders WP, Mackenzie D. The effect of
Downloaded from jada.ada.org on July 28, 2008
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
51
R E S E A R C H
smear layer on microbial coronal leakage of gutta-percha root fillings. Int Endod J 1996;29:242-8. 140. Madison S, Krell KV. Comparison of ethylenediamine tetracetic acid and sodium hypochlorite on the apical seal of endodontically treated teeth. J Endod 1984;10:499-503. 141. Timpawat S, Vongsavan N, Messer HH. Effect of removal of the smear layer on apical microleakage. J Endod 2001;27:351-3. 142. Loel DA. Use of acid cleanser in endodontic therapy. JADA 1975;90:148-51. 143. Gutirrez JH, Herrera VR, Berg EH, Villena F, Jofr A. The risk of intentional dissolution of the smear layer after mechanical preparation of root canals. Oral Surg Oral Med Oral Pathol 1990;70:96-108. 144. Pallars A, Faus V, Glickman GN. The adaptation of mechanically softened gutta-percha to the canal walls in the presence or absence of smear layer: a scanning electron microscopic study. Int Endod J 1995;28:266-9. 145. Kouvas V, Liolios E, Vassiliadis L, Parissis-Messimeris S, Boutsioukis A. Influence of smear layer depth of penetration of three endodontic sealers: an SEM study. Endod Dent Traumatol 1998; 14:191-5. 146. Genoglu N, Samani S, Gnday M. Dentinal wall adaptation of thermoplasticized gutta-percha in the absence or presence of smear layer: a scanning electron microscopic study. J Endod 1993;19:558-62. 147. Brannstrm M. Smear layer: pathological and treatment considerations. Oper Dent 1984;3(supplement):35-42. 148. Pashley DH. Smear layer: physiological considerations. Oper Dent 1984;3(supplement):13-29.
149. Georgopoulou M, Anastassiadis P, Sykaras S. Pain after chemomechanical preparation. Int Endod J 1996;19:309-14. 150. Hargreaves KM, Hutter JW. Endodontic pharmacology. In: Cohen S, Burns R, eds. Pathways of the pulp. St Louis: Mosby; 2002:665-82. 151. Holstein A, Hargreaves KM, Neiderman R. Evaluation of NSAIDs for treating post-endodontic pain: a systematic review. Endod Topics 2002;3:3-13. 152. Reader A, Nusstein J. Local anesthesia for endodontic pain. Endod Topics 2002;3:14-30. 153. Hargreaves KM, Keiser K. Local anesthetic failure in endodontics: mechanisms and management. Endod Topics 2002;1:26-39. 154. Khemaleelakul S, Baumgartner JC, Pruksakorn S. Identification of bacteria in acute endodontic infections and their antimicrobial susceptibility. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:746-55. 155. Baumgartner JC, Xia T. Antibiotic susceptibility of bacteria associated with endodontic abscesses. J Endod 2003;29:44-7. 156. Fouad AF, Barry J, Caimano M, et al. PCR-based identification of bacteria associated with endodontic infections. J Clin Microbiol 2002;40:3223-31. 157. Nagle D, Reader A, Beck M, Weaver J. Effect of systemic penicillin on pain in untreated irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:636-40. 158. Ehrich D, Lundgren J, Dionne R, Nicoll B, Hutter J. Comparison of triazolam, diazepam and placebo as outpatient oral premedication for endodontic patients. J Endod 1997;23:181-4.
Downloaded from jada.ada.org on July 28, 2008
52
JADA, Vol. 136, January 2005 Copyright 2005 American Dental Association. All rights reserved.
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- TG 9780060598242Document12 pagesTG 9780060598242Diego Escobar0% (1)
- Lessons Learned in Startup and Commissioning of Simple Cycle and Combined Cycle Combustion Turbine PlantsDocument114 pagesLessons Learned in Startup and Commissioning of Simple Cycle and Combined Cycle Combustion Turbine PlantsTerry A. Waldrop50% (4)
- Historian's Craft - Early Modern Europe, Darnton, Burke, Historical Anthropology and MentalitiesDocument6 pagesHistorian's Craft - Early Modern Europe, Darnton, Burke, Historical Anthropology and MentalitiesAbhinava GoswamiNo ratings yet
- ReleaseNotes 30101R1 131015Document10 pagesReleaseNotes 30101R1 131015pnh mcsaNo ratings yet
- EBOOK IDEO - HCD - ToolKit PDFDocument200 pagesEBOOK IDEO - HCD - ToolKit PDFangy_brooksNo ratings yet
- Fukuoka - Serene Green Roof of JapanDocument7 pagesFukuoka - Serene Green Roof of JapanJo ChanNo ratings yet
- Discussion QuestionsDocument9 pagesDiscussion QuestionsyourhunkieNo ratings yet
- Windows Scripting ComponentsDocument100 pagesWindows Scripting ComponentsyoucansuxmeNo ratings yet
- Pak Emergency Sukkur PDFDocument58 pagesPak Emergency Sukkur PDFNaeemullahNo ratings yet
- Micro Lab Act 2Document3 pagesMicro Lab Act 2RHINROMENo ratings yet
- Survey CompressedDocument394 pagesSurvey CompressedAjay PakhareNo ratings yet
- Genome Editing Medical PowerPoint TemplatesDocument48 pagesGenome Editing Medical PowerPoint TemplatesFirewall ElektroteknikNo ratings yet
- Form IR Civil Proyek PLTMG MERAUKE-20 MW (Contoh)Document94 pagesForm IR Civil Proyek PLTMG MERAUKE-20 MW (Contoh)Ramdan Pramedis SetyaNo ratings yet
- SICK DT35 Setup InstructionsDocument6 pagesSICK DT35 Setup InstructionsTalicni TomNo ratings yet
- Q4W1 WW Home-Based Task PDFDocument2 pagesQ4W1 WW Home-Based Task PDFTintin MorjiaNo ratings yet
- Acoustical Determinations On A Composite Materials (Extruded Polystyrene Type/ Cork)Document6 pagesAcoustical Determinations On A Composite Materials (Extruded Polystyrene Type/ Cork)pinoyarkiNo ratings yet
- Data Profiling OverviewDocument11 pagesData Profiling OverviewyprajuNo ratings yet
- Ctenocephalides Felis Felis vs. Ctenocephalides Canis (Siphonaptera: Pulicidae) : Some Issues in Correctly Identify These SpeciesDocument11 pagesCtenocephalides Felis Felis vs. Ctenocephalides Canis (Siphonaptera: Pulicidae) : Some Issues in Correctly Identify These SpeciesstfnhmwnNo ratings yet
- Educational PhilosophyDocument2 pagesEducational Philosophyapi-393451535No ratings yet
- Method Statement For Installation of Access ScafoldingDocument9 pagesMethod Statement For Installation of Access Scafoldingbureau servicesNo ratings yet
- Cisco TCL IvrDocument256 pagesCisco TCL IvrKarol HermickiNo ratings yet
- TCR PDF Spring 2013 Vol 25 No 1Document224 pagesTCR PDF Spring 2013 Vol 25 No 1Teresinha Pereira100% (1)
- Vivek TiwariDocument4 pagesVivek TiwariMehul ThakorNo ratings yet
- Shopping Centres, 10?FIRE?ENGINEERING ?CASE? STUDIES? IN? FINLAND?Document52 pagesShopping Centres, 10?FIRE?ENGINEERING ?CASE? STUDIES? IN? FINLAND?Bambang Setyo UtomoNo ratings yet
- Animals Grow Hessa Science: Students Will Need To Be Familiar With The Vocabulary WordsDocument4 pagesAnimals Grow Hessa Science: Students Will Need To Be Familiar With The Vocabulary WordsHessa MohammedNo ratings yet
- Flame Resistant Conveyor Belts To EN 14973 and EN 12882Document6 pagesFlame Resistant Conveyor Belts To EN 14973 and EN 12882luis martinezNo ratings yet
- Cover Letter For Content Writer With No ExperienceDocument6 pagesCover Letter For Content Writer With No Experiencebcrqhr1n100% (2)
- Credit Card Customer AnalysisDocument18 pagesCredit Card Customer AnalysisBetka AbNo ratings yet
- Fundamentals of ProbabilityDocument58 pagesFundamentals of Probabilityhien05No ratings yet
- Leadership Course OutlineDocument3 pagesLeadership Course OutlineKashif Mahmood100% (2)