You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Simplified Passover Dinner Service For KidsDocument6 pagesSimplified Passover Dinner Service For KidsPastor Jeanne100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 01the Other Man by R K LilleyDocument214 pages01the Other Man by R K LilleyAli Baba100% (5)
- Counseling Techniques FINAL 11-12-08Document1 pageCounseling Techniques FINAL 11-12-08rudolfpeterssonNo ratings yet
- Engine Test Bed: SolteqDocument4 pagesEngine Test Bed: SolteqrudolfpeterssonNo ratings yet
- ANSTDocument28 pagesANSTrudolfpeterssonNo ratings yet
- 1.3 Disaster Management: Impact of TsunamiDocument12 pages1.3 Disaster Management: Impact of TsunamirudolfpeterssonNo ratings yet
- 24x7 PHC TN ModifiedDocument33 pages24x7 PHC TN Modifiedrudolfpetersson80% (5)
- 2012 Holidays by Location1Document3 pages2012 Holidays by Location1rudolfpeterssonNo ratings yet
- Appendix: I. IndicationsDocument2 pagesAppendix: I. IndicationsrudolfpeterssonNo ratings yet
- 05 N002 28713Document20 pages05 N002 28713rudolfpeterssonNo ratings yet
- 49CDocument154 pages49Crudolfpetersson100% (2)
- Die Validation of Fuel Tank Using: Hyperform 7.0Document22 pagesDie Validation of Fuel Tank Using: Hyperform 7.0rudolfpeterssonNo ratings yet
- Design Engineer Fluid Handling Crane Pumps & Systems, Inc. Piqua, Ohio Engineering Manager OperationsDocument2 pagesDesign Engineer Fluid Handling Crane Pumps & Systems, Inc. Piqua, Ohio Engineering Manager OperationsrudolfpeterssonNo ratings yet
- Functional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueseDocument6 pagesFunctional Assessment of Cancer Therapy-Brain Questionnaire: Translation and Linguistic Adaptation To Brazilian PortugueserudolfpeterssonNo ratings yet
- Assembly DrawingDocument55 pagesAssembly DrawingKantharaj ChinnappaNo ratings yet
- A Bibliography of The History of Child ADocument219 pagesA Bibliography of The History of Child AKonstantinos Mantas100% (2)
- Chapter 3 Chemical Bonding and StructureDocument11 pagesChapter 3 Chemical Bonding and StructureTilak K CNo ratings yet
- Feeding CowDocument8 pagesFeeding CowGigiPetreaNo ratings yet
- G.O.Ms - No. 45 Dated:09-09-2016 Read The FollowingDocument40 pagesG.O.Ms - No. 45 Dated:09-09-2016 Read The Followingsto kaikaluruNo ratings yet
- Baxi Duo Tec Hea Installation GuideDocument60 pagesBaxi Duo Tec Hea Installation GuideDana LoreNo ratings yet
- Contractor Management ProcedureDocument13 pagesContractor Management ProcedureNaba majeadNo ratings yet
- Soal Cloze Test Explanation - Global WarmingDocument2 pagesSoal Cloze Test Explanation - Global WarmingPanci SeSbs d'NightflierNo ratings yet
- Fundamentals of Male Infertility First Edition Sherman SilberDocument211 pagesFundamentals of Male Infertility First Edition Sherman Silberlgrv94No ratings yet
- Dialog Drama B. IngDocument5 pagesDialog Drama B. IngMustikaArfahNo ratings yet
- The Body ShopDocument3 pagesThe Body ShopArwandyaz Brimandyka0% (1)
- Horticulture in HotelsDocument14 pagesHorticulture in Hotelssaikripa12133% (3)
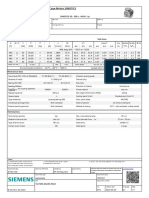
- 1LE1503-2AA43-4AA4 Datasheet enDocument1 page1LE1503-2AA43-4AA4 Datasheet enAndrei LupuNo ratings yet
- Lecture 1 Introduction To MicrobiologyDocument76 pagesLecture 1 Introduction To MicrobiologyFjNo ratings yet
- Sym Euro MX 125 (EN)Document193 pagesSym Euro MX 125 (EN)manualsym0% (1)
- Analysis of Pork Contamination in Abon Using Mitochondrial D-Loop22 Primers Using Real Time Polymerase Chain Reaction MethodDocument5 pagesAnalysis of Pork Contamination in Abon Using Mitochondrial D-Loop22 Primers Using Real Time Polymerase Chain Reaction MethodFenny AuliaNo ratings yet
- Jeevan Surabhi - 106 - 107 - 108Document3 pagesJeevan Surabhi - 106 - 107 - 108Vinay KumarNo ratings yet
- Atk FixDocument9 pagesAtk FixRama SlaluhappyNo ratings yet
- Using Wavelet Analysis To Characterize The Thermoregulatory Mechanisms of Sacral Skin Blood FlowDocument9 pagesUsing Wavelet Analysis To Characterize The Thermoregulatory Mechanisms of Sacral Skin Blood Flowh6j4vsNo ratings yet
- Group 6 - PRW301 - AS2020 - Final ReportDocument20 pagesGroup 6 - PRW301 - AS2020 - Final ReportPema ChodenNo ratings yet
- Discharge Process SynopsisDocument7 pagesDischarge Process Synopsisdrbhavya250% (1)
- Discover - Mar - Apr 2022Document68 pagesDiscover - Mar - Apr 2022BalaramanNo ratings yet
- دليل صيانة الجسور و الانفاقenDocument454 pagesدليل صيانة الجسور و الانفاقensidiq7No ratings yet
- Analysis and Prevention of Bearing FailuresDocument76 pagesAnalysis and Prevention of Bearing Failurestahazeeshan100% (1)
- Chapter I PDFDocument13 pagesChapter I PDFKeerthi PNo ratings yet
- Delegate Scott Surovell Letter Regarding 2015 FCPS School Boundary CIP LetterDocument2 pagesDelegate Scott Surovell Letter Regarding 2015 FCPS School Boundary CIP LetterScott A. SurovellNo ratings yet
- Construction Company Profile TemplateDocument1 pageConstruction Company Profile TemplateAshutosh Singh100% (1)
- Dynamo Industries - AssignmentDocument2 pagesDynamo Industries - AssignmentAhsan ShakirNo ratings yet
- The - Week.usa May.12 2017 p2pDocument46 pagesThe - Week.usa May.12 2017 p2pMadalinedgarNo ratings yet