You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Prolonged Labour: Mrs. Shwetha Rani C.MDocument24 pagesProlonged Labour: Mrs. Shwetha Rani C.MSanthosh.S.U100% (1)
- Lecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFDocument37 pagesLecture 12-National Global Psychosocial Problem-Dr. Mahar Agusno, SP - KJ (K) (2020) PDFstefany huangNo ratings yet
- DA Form 5164-R Hands-On EvaluationDocument1 pageDA Form 5164-R Hands-On EvaluationLuke Layton100% (1)
- Alternative Method For Fabrication of Power ArmDocument2 pagesAlternative Method For Fabrication of Power ArmVikas VatsNo ratings yet
- Facial AnatomyDocument11 pagesFacial AnatomySneha SthaNo ratings yet
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDocument6 pagesVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsNo ratings yet
- The Anatomical Basis For Surgical Preservation of Temporal MuscleDocument6 pagesThe Anatomical Basis For Surgical Preservation of Temporal Musclekurtwaldhaim22No ratings yet
- Evoked PotentialDocument6 pagesEvoked PotentialVikas VatsNo ratings yet
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDocument2 pagesBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDocument17 pagesPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsNo ratings yet
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDocument9 pagesComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsNo ratings yet
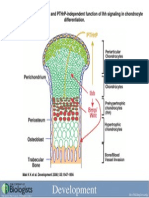
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Document1 pageDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsNo ratings yet
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNo ratings yet
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Document5 pages1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsNo ratings yet
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsNo ratings yet
- AIR DROP EXAMنسختي PDFDocument35 pagesAIR DROP EXAMنسختي PDFYara AlmouallemNo ratings yet
- Tromboembolismo Pulmonar Manejo PDFDocument7 pagesTromboembolismo Pulmonar Manejo PDFGeovannaHGNo ratings yet
- MAPEH10 Module 4Document36 pagesMAPEH10 Module 4albaystudentashleyNo ratings yet
- Impact of Magnet Disgnation On Hcahps Scores FinalDocument19 pagesImpact of Magnet Disgnation On Hcahps Scores Finalapi-257580555No ratings yet
- Clinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysisDocument8 pagesClinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysissamNo ratings yet
- Tsoukaki 2012Document8 pagesTsoukaki 2012Marina JoelNo ratings yet
- Nej M CPC 2103461Document10 pagesNej M CPC 2103461monaNo ratings yet
- Progress of Molecular Targeted Therapies For ProstatecancersDocument13 pagesProgress of Molecular Targeted Therapies For ProstatecancersNenad MladenovicNo ratings yet
- Phytopharmaceuticals: A New Class of Drug in India: June 2018Document12 pagesPhytopharmaceuticals: A New Class of Drug in India: June 2018Mahendran NNo ratings yet
- Gabapentina en GatosDocument9 pagesGabapentina en GatosSócrates MillmanNo ratings yet
- Rash DDDocument5 pagesRash DDSyed Moin HassanNo ratings yet
- 1 Extemporaneous Compounding - HPREDocument2 pages1 Extemporaneous Compounding - HPREKianna Marie MuyotNo ratings yet
- 240-Article Text-484-3-10-20210620Document7 pages240-Article Text-484-3-10-20210620denny yusufNo ratings yet
- Medication Information For Parents and Teachers: Amphetamine-Dexedrine, Procentra, Zenzedi, Adderall, VyvanseDocument10 pagesMedication Information For Parents and Teachers: Amphetamine-Dexedrine, Procentra, Zenzedi, Adderall, VyvanseMonique WrightNo ratings yet
- Mir & MCRDocument1 pageMir & MCRMhmoud NabehNo ratings yet
- Down SyndromeDocument20 pagesDown SyndromeJessa DiñoNo ratings yet
- Unit IvDocument10 pagesUnit IvmasorNo ratings yet
- EMSI What Is A Paramed E0099 - V2 12-13 EDocument2 pagesEMSI What Is A Paramed E0099 - V2 12-13 Erina cNo ratings yet
- Evaluation of Condylar Morphology Using Panoramic RadiographyDocument4 pagesEvaluation of Condylar Morphology Using Panoramic RadiographyRifqaNo ratings yet
- Terapi Jus Semangka - 10-20210203Document10 pagesTerapi Jus Semangka - 10-20210203Mhyla MusaNo ratings yet
- Olana Gadisa Edited Proposal-1Document29 pagesOlana Gadisa Edited Proposal-1kelid IbrahimNo ratings yet
- IPADocument27 pagesIPACristina ToaderNo ratings yet
- Student ServicesDocument19 pagesStudent Servicesapi-297925543No ratings yet
- KEIZINAN - ZDocument52 pagesKEIZINAN - ZMisya SafinaNo ratings yet
- The Following T-WPS OfficeDocument6 pagesThe Following T-WPS OfficeNilam CahyaniNo ratings yet
- Notification No. SO (SC) 1-13317 Seniority List of Consultants (BS-18) 1-3-18Document51 pagesNotification No. SO (SC) 1-13317 Seniority List of Consultants (BS-18) 1-3-18IrfanNo ratings yet
- Nfpe PresentationDocument28 pagesNfpe Presentationapi-389891541No ratings yet