You might also like
- History of America Before Columbus According To Documents and Approved Authors PDFDocument878 pagesHistory of America Before Columbus According To Documents and Approved Authors PDFTy0072100% (3)
- Bayesian Cost Effectiveness Analysis With The R Package BCEA PDFDocument181 pagesBayesian Cost Effectiveness Analysis With The R Package BCEA PDFNelson Carvas JrNo ratings yet
- 2020 International Society of Hypertension Global Hypertension Practice GuidelinesDocument48 pages2020 International Society of Hypertension Global Hypertension Practice GuidelinesNicoleta Popa-FoteaNo ratings yet
- SQF Edition 8 Quick Start GuideDocument27 pagesSQF Edition 8 Quick Start Guidefourat.zarkounaNo ratings yet
- Diabetes Management: OverviewDocument20 pagesDiabetes Management: Overviewlaloo01No ratings yet
- Simulation of CO2 Capture Using MEA Scrubbing A Flowsheet Decomposition Method PDFDocument13 pagesSimulation of CO2 Capture Using MEA Scrubbing A Flowsheet Decomposition Method PDFSuprio KamalNo ratings yet
- GOUT PresentationDocument24 pagesGOUT Presentationtasneemsofi100% (1)
- Diabetes and Hypertension: A Comparative Review of Current GuidelinesDocument6 pagesDiabetes and Hypertension: A Comparative Review of Current GuidelineskartikayuanafitriNo ratings yet
- Diabetes Management in Chronic Kidney Disease: Synopsis of The 2020 KDIGO Clinical Practice GuidelineDocument14 pagesDiabetes Management in Chronic Kidney Disease: Synopsis of The 2020 KDIGO Clinical Practice Guidelinecarlos llanos florezNo ratings yet
- Clinical Evaluation of DiabetesDocument24 pagesClinical Evaluation of DiabetesDhirender KaushikNo ratings yet
- Executive Summary of The 2020 KDIGO Diabetes Management in CKD Guideline: Evidence-Based Advances in Monitoring and TreatmentDocument10 pagesExecutive Summary of The 2020 KDIGO Diabetes Management in CKD Guideline: Evidence-Based Advances in Monitoring and TreatmentAlbert Andía MamaniNo ratings yet
- ADA Guidelines 2012Document53 pagesADA Guidelines 2012Jones PessoaNo ratings yet
- Comparison Between The World Health Organization WHO and International Society of Hypertension ISH Guidelines For HypertensionDocument10 pagesComparison Between The World Health Organization WHO and International Society of Hypertension ISH Guidelines For Hypertensionkelvin pradanaNo ratings yet
- JBDS RenalGuideAbbreviated 2016Document26 pagesJBDS RenalGuideAbbreviated 2016Majid KhanNo ratings yet
- Compare WHO & ISH Guidlines HPTDocument9 pagesCompare WHO & ISH Guidlines HPTAdinda Raihana SitorusNo ratings yet
- ART Dia Care-2013 - S11-66Document56 pagesART Dia Care-2013 - S11-66LuisArroboNo ratings yet
- Dyspepsia: Scottish Intercollegiate Guidelines NetworkDocument30 pagesDyspepsia: Scottish Intercollegiate Guidelines NetworkAna Cristina IssaNo ratings yet
- Concept Paper Need Revision Guideline Clinical Investigation Medicinal Products Treatment Prevention - enDocument4 pagesConcept Paper Need Revision Guideline Clinical Investigation Medicinal Products Treatment Prevention - enSamwel OtienoNo ratings yet
- Chapter 1 IntroductionDocument3 pagesChapter 1 IntroductionIsla SpencerNo ratings yet
- Standards of Medical Care in Diabetes-2011: Merican Iabetes SsociationDocument51 pagesStandards of Medical Care in Diabetes-2011: Merican Iabetes SsociationLayane TérciaNo ratings yet
- Management of Diabetes: November 2010Document54 pagesManagement of Diabetes: November 2010Tzi Mohd ZailaniNo ratings yet
- البحثDocument43 pagesالبحثحسين علي ذيبان عليNo ratings yet
- Hypoglychemia AdultsDocument32 pagesHypoglychemia AdultsshutekiNo ratings yet
- The New NICE Guidelines For Type 2 Diabetes - A CRDocument6 pagesThe New NICE Guidelines For Type 2 Diabetes - A CRkehie HananielNo ratings yet
- Sepsis Guidelines 2012Document13 pagesSepsis Guidelines 2012Lauren WilkersonNo ratings yet
- Managing Hyperglycaemia in People With DKD - Final DraftDocument90 pagesManaging Hyperglycaemia in People With DKD - Final DraftRiched LhyneNo ratings yet
- DiabetesDocument10 pagesDiabetesRoberto HangleyNo ratings yet
- Lifestyle Modification and Hypertension Prevention: Sima Ghezelbash, Azam GhorbaniDocument6 pagesLifestyle Modification and Hypertension Prevention: Sima Ghezelbash, Azam Ghorbanineway workuNo ratings yet
- Protocol 007Document7 pagesProtocol 007hatem newishyNo ratings yet
- Frailty Jbds Ipfinal 28 10 19Document70 pagesFrailty Jbds Ipfinal 28 10 19Xylia TocaoNo ratings yet
- Lifestyle Modification and Hypertension PreventionDocument6 pagesLifestyle Modification and Hypertension PreventionFahmi Abdul HaqNo ratings yet
- Sheffield Diabetes Resource PackDocument195 pagesSheffield Diabetes Resource Packhappyman1978No ratings yet
- Management of Hyperglycaemia in Type 2 Diabetes, 2022Document42 pagesManagement of Hyperglycaemia in Type 2 Diabetes, 2022Monika Diaz KristyanindaNo ratings yet
- 2022 ADA/EASD共识报告:2型糖尿病高血糖的管理Document42 pages2022 ADA/EASD共识报告:2型糖尿病高血糖的管理李木子No ratings yet
- Cardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Document34 pagesCardiovascular Disease in CKD - FINAL DRAFT (26 May 2010)Dee DNo ratings yet
- Dyspepsia: Scottish Intercollegiate Guidelines NetworkDocument30 pagesDyspepsia: Scottish Intercollegiate Guidelines NetworkTruly Dian AnggrainiNo ratings yet
- Guideline XDocument104 pagesGuideline XcarolinapolotorresNo ratings yet
- GoutDocument5 pagesGoutJayson TrajanoNo ratings yet
- Hyper TensionDocument54 pagesHyper TensionViky SinghNo ratings yet
- Teaching of Diabetes Mellitus To Medical Students and Primary Health Care Nurses: A Family Medicine PerspectiveDocument4 pagesTeaching of Diabetes Mellitus To Medical Students and Primary Health Care Nurses: A Family Medicine Perspectivepearl_nursingNo ratings yet
- 2017 Article 531Document7 pages2017 Article 531dinimusmanNo ratings yet
- Review of The Literature On The Impact of The Functional Insulin TherapyDocument7 pagesReview of The Literature On The Impact of The Functional Insulin TherapyIJAR JOURNALNo ratings yet
- National Evidence Based Guidelines PDFDocument246 pagesNational Evidence Based Guidelines PDFNarendraNo ratings yet
- 2016 Article 42 PDFDocument8 pages2016 Article 42 PDFSandhya kumarNo ratings yet
- Standards of Medical Care in Diabetes-2011Document66 pagesStandards of Medical Care in Diabetes-2011Marcos Isai Velez SantillanNo ratings yet
- Pelumi 1Document7 pagesPelumi 1oluwasegunnathaniel0No ratings yet
- The Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionDocument40 pagesThe Hospital Management of Hypoglycaemia in Adults With Diabetes Mellitus 3rd EditionRumahSehat N-CareNo ratings yet
- Abrir Cetoacidosis 2022Document20 pagesAbrir Cetoacidosis 2022Giovanny Alexander BravoNo ratings yet
- Drugs Increased Risk of DiabetesDocument5 pagesDrugs Increased Risk of Diabetesk9cfxtdfqmNo ratings yet
- THE Canadian Hypertension Education Program Recommendations: An Annual UpdateDocument64 pagesTHE Canadian Hypertension Education Program Recommendations: An Annual Updatenurendah90No ratings yet
- Standards of Medical Care in Diabetes-2011: Merican Iabetes SsociationDocument51 pagesStandards of Medical Care in Diabetes-2011: Merican Iabetes SsociationYazmin CamachoNo ratings yet
- Cetoacidosis 2022Document20 pagesCetoacidosis 2022David RojasNo ratings yet
- Executive Summary of The 2020 Clinical Practice Guidelines For The Management of Hypertension in The PhilippinesDocument30 pagesExecutive Summary of The 2020 Clinical Practice Guidelines For The Management of Hypertension in The PhilippinesBhaby Cen-cenNo ratings yet
- Evaluation of Pharmacotherapies For Alcoholic Liver Disease: A Retrospective Real-World Evidence StudyDocument13 pagesEvaluation of Pharmacotherapies For Alcoholic Liver Disease: A Retrospective Real-World Evidence StudyEditor ERWEJNo ratings yet
- Standards of Medical Care in Diabetes: Merican Iabetes SsociationDocument33 pagesStandards of Medical Care in Diabetes: Merican Iabetes Ssociationdavid-lo-512No ratings yet
- Estandares de Manejo AdaDocument38 pagesEstandares de Manejo AdaHERACLITONo ratings yet
- Homeopathic Treatment of Acute GoutDocument5 pagesHomeopathic Treatment of Acute GoutAgustinusNo ratings yet
- Management of Hyperglycaemia and Steroid (Glucocorticoid) TherapyDocument28 pagesManagement of Hyperglycaemia and Steroid (Glucocorticoid) TherapyLatifatu ChoirunisaNo ratings yet
- Biologics Guidelines 2009Document33 pagesBiologics Guidelines 2009amimusriNo ratings yet
- Discover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingFrom EverandDiscover The Best Exercises For Overall Health & Longevity - Based On The Teachings Of Dr. Andrew Huberman: The Ultimate Workout Guide For Lifelong Well-BeingNo ratings yet
- Hypertension and 24-hour Ambulatory Blood Pressure MonitoringFrom EverandHypertension and 24-hour Ambulatory Blood Pressure MonitoringNo ratings yet
- 5 Energy ManagementDocument1 page5 Energy ManagementDibyo SetiawanNo ratings yet
- Assignment 1Document2 pagesAssignment 1Nayyar AbbasiNo ratings yet
- AGI 400 Series Data Sheet 4921240564 UKDocument19 pagesAGI 400 Series Data Sheet 4921240564 UKEdwin PinzonNo ratings yet
- PsychosesDocument32 pagesPsychosesAnonymous zxTFUoqzklNo ratings yet
- Vendor Document Cover SheetDocument11 pagesVendor Document Cover SheetSagar SawantNo ratings yet
- R.K. Anand Contempt Delhi HC JudgementDocument112 pagesR.K. Anand Contempt Delhi HC JudgementSampath BulusuNo ratings yet
- Wa0041Document2 pagesWa0041Muthu KumarNo ratings yet
- Using Techniques On Seeking, Screening, and Seizing OpportunitiesDocument8 pagesUsing Techniques On Seeking, Screening, and Seizing OpportunitiesJustine Evasco RubiaNo ratings yet
- Statistical Physics Phy632-Tutorial: Sharifah Hafizah Binti Syed Ab AzizDocument26 pagesStatistical Physics Phy632-Tutorial: Sharifah Hafizah Binti Syed Ab AzizSharifahHafizahAl-jufNo ratings yet
- Workshop On Previewing - CECARDocument12 pagesWorkshop On Previewing - CECARestefaany tejada100% (2)
- TestDocument4 pagesTestAlina DushachenkoNo ratings yet
- Negative Effects of Social Media AddictionDocument2 pagesNegative Effects of Social Media AddictionTubagus Fikih AriansyahNo ratings yet
- Coverpage BLDG Projects F.Y. 2021Document4 pagesCoverpage BLDG Projects F.Y. 2021Adrian PachecoNo ratings yet
- Approach SlabDocument2 pagesApproach SlabMahmood Mufti100% (1)
- Flsmidth Private Limited: Quality Assurance Plan of Exciter CasingDocument5 pagesFlsmidth Private Limited: Quality Assurance Plan of Exciter CasingMohammad AdilNo ratings yet
- Esr 2653Document9 pagesEsr 2653Uğur ErdoğanNo ratings yet
- International Financial Regulation Seminar QuestionsDocument2 pagesInternational Financial Regulation Seminar QuestionsNicu BotnariNo ratings yet
- You Are The ReasonDocument7 pagesYou Are The ReasonSindi Ghassani SabilaNo ratings yet
- Lab-Journal Compiler ConstructionDocument20 pagesLab-Journal Compiler ConstructionAbdullah ArshadNo ratings yet
- Gallipoli Diary, Volume 2 by Hamilton, Ian, 1853-1947Document191 pagesGallipoli Diary, Volume 2 by Hamilton, Ian, 1853-1947Gutenberg.orgNo ratings yet
- QUIZ ENGCOM 2 - Week 4Document2 pagesQUIZ ENGCOM 2 - Week 4Amin sanNo ratings yet
- BOSS GLOBAL CONCEPTS LTD - AML Policy-UpdatedDocument46 pagesBOSS GLOBAL CONCEPTS LTD - AML Policy-UpdatedtwaseemdttNo ratings yet
- Synapse: I. Anatomical TypesDocument5 pagesSynapse: I. Anatomical TypesAswin AjayNo ratings yet
- Toaz - Info Chapter 6 PRDocument14 pagesToaz - Info Chapter 6 PRMelissa Indah FiantyNo ratings yet
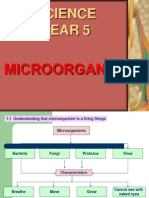
- Science Year 5: MicroorganismsDocument8 pagesScience Year 5: MicroorganismscthanifahNo ratings yet
- Aim Efi Euro1 100 EngDocument8 pagesAim Efi Euro1 100 EngManuel RodriguezNo ratings yet