You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Parrino 2e PowerPoint Review Ch13Document55 pagesParrino 2e PowerPoint Review Ch13Khadija AlkebsiNo ratings yet
- Lab 3 Grip Strength LabDocument3 pagesLab 3 Grip Strength LabSofwan JuewekNo ratings yet
- COBIT 5 Poster 1 Transforming Stakeholder PDFDocument1 pageCOBIT 5 Poster 1 Transforming Stakeholder PDFLuis MessiasNo ratings yet
- The Senior Voice - January 2010Document16 pagesThe Senior Voice - January 2010The Senior VoiceNo ratings yet
- Support Material / Material de Apoyo Learning Activity 3 / Actividad de Aprendizaje 3Document6 pagesSupport Material / Material de Apoyo Learning Activity 3 / Actividad de Aprendizaje 3Alexandra ChavarroNo ratings yet
- 100 Persons of The CenturyDocument1 page100 Persons of The CenturyAaron LawlerNo ratings yet
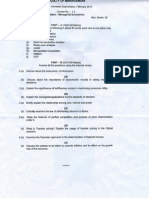
- Managerial Economics MBA OU Question PaperDocument11 pagesManagerial Economics MBA OU Question Paperratansrikanth75% (4)
- A Commerce in ButterfliesDocument6 pagesA Commerce in ButterfliesJenika Jean ReanzaresNo ratings yet
- Coronary Artery DiseaseDocument7 pagesCoronary Artery Diseasejmar767No ratings yet
- Pass 1 Assembler in CDocument15 pagesPass 1 Assembler in CEkta Singh85% (13)
- High-pH-Magnesium Coagulation-Flocculation in Wastewater TreatmentDocument16 pagesHigh-pH-Magnesium Coagulation-Flocculation in Wastewater TreatmentAJITH SNo ratings yet
- Scribed Thomas Hardy Afterwards AnalysisDocument17 pagesScribed Thomas Hardy Afterwards AnalysisShanta PalNo ratings yet
- Kath Bocalan - PR1 - Q1 - Activity-1Document4 pagesKath Bocalan - PR1 - Q1 - Activity-1Kath BocalanNo ratings yet
- Mark M Calban MD MPM-HSDDocument58 pagesMark M Calban MD MPM-HSDZllison Mae Teodoro Mangabat100% (1)
- PoolSpaN USPHDocument47 pagesPoolSpaN USPHpetar.petrov.111964No ratings yet
- RAFAEL H. GALVEZ Et Al. Vs CADocument2 pagesRAFAEL H. GALVEZ Et Al. Vs CAAnsai CaluganNo ratings yet
- Airbus AC A321 Jun2012Document484 pagesAirbus AC A321 Jun2012Megan SotoNo ratings yet
- Double Jeopardy CaseDocument7 pagesDouble Jeopardy CasePing KyNo ratings yet
- He Imes Eader: Obama Promises Rigorous ReviewDocument36 pagesHe Imes Eader: Obama Promises Rigorous ReviewThe Times LeaderNo ratings yet
- Business EtiquetteDocument24 pagesBusiness Etiquettesee1tearNo ratings yet
- AAF007 CORPurchaseAAInstallment V03Document2 pagesAAF007 CORPurchaseAAInstallment V03Jerson OboNo ratings yet
- Heung 2012Document11 pagesHeung 2012Luis Jhonny Dávila ValderaNo ratings yet
- Intercultural Communication (By O.L. Kocheva)Document21 pagesIntercultural Communication (By O.L. Kocheva)ЕкатеринаNo ratings yet
- MKT 380 - Answers To Test 2 Review QuestionsDocument7 pagesMKT 380 - Answers To Test 2 Review QuestionsShannon UeberflussNo ratings yet
- PENGARUH EKSTRAK DAUN KELOR (Moringa Oleifera L.) Terhadap Kualitas YoghurtDocument8 pagesPENGARUH EKSTRAK DAUN KELOR (Moringa Oleifera L.) Terhadap Kualitas YoghurtChaaNo ratings yet
- Culinary Test Exam 1Document18 pagesCulinary Test Exam 1Sapna SharmaNo ratings yet
- El Noticiero RubricDocument2 pagesEl Noticiero RubricAlfredo CruzNo ratings yet
- Case DigestsDocument209 pagesCase DigestsEloisa Katrina MadambaNo ratings yet
- And The Day of Hunain Urgent Message To The Revolutionaries of LibyaDocument7 pagesAnd The Day of Hunain Urgent Message To The Revolutionaries of LibyadayofhunainNo ratings yet
- Muhajir DiasporaDocument10 pagesMuhajir DiasporaneoindusNo ratings yet