You might also like
- Adult Major Depressive Disorder (MDD) : Suicide Risk AssessmentDocument4 pagesAdult Major Depressive Disorder (MDD) : Suicide Risk Assessmentjuloc34No ratings yet
- PSO - Largo Plazo - Switch Kim PappDocument13 pagesPSO - Largo Plazo - Switch Kim Pappjuloc34No ratings yet
- CXG 055eDocument3 pagesCXG 055eKishor MaloreNo ratings yet
- Start Now Before A PotDocument2 pagesStart Now Before A Potjuloc34No ratings yet
- CXG 055eDocument3 pagesCXG 055eKishor MaloreNo ratings yet
- Lahiri 2 - Unlocked PDFDocument5 pagesLahiri 2 - Unlocked PDFjuloc34No ratings yet
- Lahiri 2 - Unlocked PDFDocument5 pagesLahiri 2 - Unlocked PDFjuloc34No ratings yet
- Hospital Admission For Heart Failure: An Opportunity To Optimize Heart Failure Therapy?Document27 pagesHospital Admission For Heart Failure: An Opportunity To Optimize Heart Failure Therapy?juloc34No ratings yet
- Neuropsychiatric Manifestations of Vitamin B12 and Folate Deficiencies: Data From An Inpatient Psychiatric DepartmentDocument2 pagesNeuropsychiatric Manifestations of Vitamin B12 and Folate Deficiencies: Data From An Inpatient Psychiatric Departmentjuloc34No ratings yet
- RTC-SW 2014 10 P Anaemia in Pregnancy GuidelineDocument5 pagesRTC-SW 2014 10 P Anaemia in Pregnancy GuidelineShiina LeeNo ratings yet
- Why, When, and How: Seize The Moment To Optimize Treatment For Each Patient With Heart FailureDocument7 pagesWhy, When, and How: Seize The Moment To Optimize Treatment For Each Patient With Heart Failurejuloc34No ratings yet
- Joint Statement ESPGHANESPACI1999Document8 pagesJoint Statement ESPGHANESPACI1999juloc34No ratings yet
- Comparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-AcquiredDocument9 pagesComparative Study of Levofloxacin and Amoxycillin/clavulanic Acid in Adults With Mild-To-Moderate Community-Acquiredjuloc34No ratings yet
- Baker Et Al-2003-Arthritis & Rheumatism PDFDocument13 pagesBaker Et Al-2003-Arthritis & Rheumatism PDFjuloc34No ratings yet
- Fucosylated Human Milk OligosaccharidesDocument8 pagesFucosylated Human Milk Oligosaccharidesjuloc34No ratings yet
- ACR 2011 Clinicians GuideDocument7 pagesACR 2011 Clinicians Guidejuloc34No ratings yet
- 87ri7 113Document11 pages87ri7 113juloc34No ratings yet
- IDF - Atlas 2015 - UK PDFDocument144 pagesIDF - Atlas 2015 - UK PDFjuloc34No ratings yet
- 731 1457 1 PBDocument4 pages731 1457 1 PBjuloc34No ratings yet
- A134 oct06DunnS335toS344 06Document10 pagesA134 oct06DunnS335toS344 06juloc34No ratings yet
- 8w812 Outdoor Photographer August 2015 HQ PDFDocument92 pages8w812 Outdoor Photographer August 2015 HQ PDFjuloc34No ratings yet
- Actualización Guías Tratamiento Ar Acr 2012Document15 pagesActualización Guías Tratamiento Ar Acr 2012Felipe VasquezNo ratings yet
- Effect of Iron-Deficiency Anemia On Cognitive Skills and Neuromaturation in Infancy and ChildhoodDocument7 pagesEffect of Iron-Deficiency Anemia On Cognitive Skills and Neuromaturation in Infancy and Childhoodjuloc34No ratings yet
- Efficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC StudyDocument1 pageEfficacy and Safety of Vismodegib in Patients With Advanced Basal Cell Carcinoma (BCC) : 12-Month Update of The ERIVANCE BCC Studyjuloc34No ratings yet
- Residual Neuromuscular Block: Lessons Unlearned. Part II: Methods To Reduce The Risk of Residual WeaknessDocument12 pagesResidual Neuromuscular Block: Lessons Unlearned. Part II: Methods To Reduce The Risk of Residual Weaknessjuloc34No ratings yet
- Iron Metabolism and Requirements in Early Childhood: Do We Know Enough?: A Commentary by The ESPGHAN Committee On NutritionDocument9 pagesIron Metabolism and Requirements in Early Childhood: Do We Know Enough?: A Commentary by The ESPGHAN Committee On Nutritionjuloc34No ratings yet
- Residual Neuromuscular Block: Lessons Unlearned. Part II: Methods To Reduce The Risk of Residual WeaknessDocument12 pagesResidual Neuromuscular Block: Lessons Unlearned. Part II: Methods To Reduce The Risk of Residual Weaknessjuloc34No ratings yet
- Hyman Roma IIIDocument8 pagesHyman Roma IIIjuloc34No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chan VS ChanDocument2 pagesChan VS ChanEduard RiparipNo ratings yet
- A Copy of The Formal Complaint Filed by The Texas Medical Board Against Dr. Mary BowdenDocument12 pagesA Copy of The Formal Complaint Filed by The Texas Medical Board Against Dr. Mary BowdenHouston ChronicleNo ratings yet
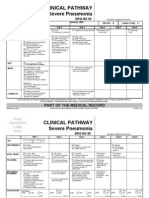
- Clinical Pathways Severe PneumoniaDocument2 pagesClinical Pathways Severe PneumoniaaandakuNo ratings yet
- Medical Records, Insurance, and ContractsDocument32 pagesMedical Records, Insurance, and ContractsBernard Kwaku OkaiNo ratings yet
- Career Test Result: Personality Types and Holland CodesDocument4 pagesCareer Test Result: Personality Types and Holland Codesapi-307132793No ratings yet
- QPS Sample GuidelinesDocument23 pagesQPS Sample GuidelinesSafiqulatif AbdillahNo ratings yet
- RCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Document2 pagesRCL Employment Medical Examination Form A (New-Returning) Revised 2015-03Ahmad ShodiqNo ratings yet
- NSG Process-Chitra MamDocument44 pagesNSG Process-Chitra MamJalajarani AridassNo ratings yet
- Apex Manual RPOCDocument70 pagesApex Manual RPOCtanisha100% (1)
- Ethics Professional Conduct: American Dental AssociationDocument24 pagesEthics Professional Conduct: American Dental AssociationMavisNo ratings yet
- Short Term Training Curriculum Handbook PHLEBOTOMISTDocument33 pagesShort Term Training Curriculum Handbook PHLEBOTOMISTrokdeNo ratings yet
- Activity Design June 2017 Program Title: Iclinicsys Training RationaleDocument2 pagesActivity Design June 2017 Program Title: Iclinicsys Training Rationalepedrong dodongNo ratings yet
- Pad 411 - Health AdministrationDocument177 pagesPad 411 - Health AdministrationMuttaka Turaki Gujungu100% (1)
- March 13, 2015 Letter To Dr. Kristina Borror at OHRPDocument4 pagesMarch 13, 2015 Letter To Dr. Kristina Borror at OHRPLeighTurnerNo ratings yet
- Little Harwood Health Centre Practice LeafletDocument5 pagesLittle Harwood Health Centre Practice Leafletkovi mNo ratings yet
- The Wayland News July 2011Document20 pagesThe Wayland News July 2011Julian HornNo ratings yet
- J Applied Clin Med Phys - 2022 - Fisher - AAPM Medical Physics Practice Guideline 12 A Fluoroscopy Dose Management-1Document19 pagesJ Applied Clin Med Phys - 2022 - Fisher - AAPM Medical Physics Practice Guideline 12 A Fluoroscopy Dose Management-1Roshi_11No ratings yet
- Anecdotal RecordsDocument21 pagesAnecdotal Recordsvanshika thukral80% (10)
- Know Your Hospital: Submitted by Joyita ChatterjeeDocument13 pagesKnow Your Hospital: Submitted by Joyita ChatterjeeJoyita ChatterjeeNo ratings yet
- Literature Review Article Electroinc Medical Records Stimulation For Nursing Students 3 5Document2 pagesLiterature Review Article Electroinc Medical Records Stimulation For Nursing Students 3 5Andrea TylerNo ratings yet
- Pinamalayan Doctors' Hospital: Policies and ProcedureDocument9 pagesPinamalayan Doctors' Hospital: Policies and Procedurefredie rick luceNo ratings yet
- Proctoring Policy 5 12Document6 pagesProctoring Policy 5 12Dwi cahyaniNo ratings yet
- Secondary Use of Electronic Health RecordDocument19 pagesSecondary Use of Electronic Health RecordRaksha hiwaNo ratings yet
- MLC Area 02 - Medical Fitness - ILO - 2011-00-00 - Guidelines On The Medical Examinations of SeafarersDocument69 pagesMLC Area 02 - Medical Fitness - ILO - 2011-00-00 - Guidelines On The Medical Examinations of SeafarersMilan ChaddhaNo ratings yet
- Relevant Ethico-Legal GuidelinesDocument17 pagesRelevant Ethico-Legal GuidelinesPauline M.No ratings yet
- Healthcare Administration Resume ExamplesDocument7 pagesHealthcare Administration Resume Examplesafayememn100% (2)
- Evaluation of California Non-Comprehensive Death File Against National Death IndexDocument14 pagesEvaluation of California Non-Comprehensive Death File Against National Death IndexCONSTANZA TERESA BERNA ARAYANo ratings yet
- WA Health Consent To Treatment Policy: Better Health Better Care Better ValueDocument42 pagesWA Health Consent To Treatment Policy: Better Health Better Care Better ValueprabhaNo ratings yet
- Are Electronic Medical Records A Cure For Health Care?Document4 pagesAre Electronic Medical Records A Cure For Health Care?Sanjay PudasainiNo ratings yet