You might also like
- Prevalence and Impact of Pain Among Older Adults in The United StatesDocument9 pagesPrevalence and Impact of Pain Among Older Adults in The United StatesLucas TarquiNo ratings yet
- JNR 23841Document11 pagesJNR 23841Ablfazl KianiNo ratings yet
- Physical Therapy Intervention For Women With Dyspareunia: A Randomized Clinical TrialDocument32 pagesPhysical Therapy Intervention For Women With Dyspareunia: A Randomized Clinical TrialFERNANDA SILVEIRANo ratings yet
- 2016 Psychological Stress in Early Life As A Predisposing Factor For The Development of Chronic Pain. Clinical and Preclinical Evidence and Neurobiological MechanismDocument14 pages2016 Psychological Stress in Early Life As A Predisposing Factor For The Development of Chronic Pain. Clinical and Preclinical Evidence and Neurobiological MechanismCristian OyarzoNo ratings yet
- Sullivan Feb 2000Document15 pagesSullivan Feb 2000Ummu SolihahNo ratings yet
- Sex Differences and Mechanisms of Muscle Pain: Luis F Queme and Michael P JankowskiDocument6 pagesSex Differences and Mechanisms of Muscle Pain: Luis F Queme and Michael P JankowskiBeto BaezaNo ratings yet
- Avances de La Busqueda de BibliografiaDocument21 pagesAvances de La Busqueda de BibliografiaMaria ChisaNo ratings yet
- Yin Paper Im 2020 FinalDocument19 pagesYin Paper Im 2020 Finalapi-512426092No ratings yet
- Women in Chronic Pain Sense of Control andDocument11 pagesWomen in Chronic Pain Sense of Control andEmilie BergeronNo ratings yet
- OA biolSexDiffDocument12 pagesOA biolSexDiffSex & Gender Women's Health CollaborativeNo ratings yet
- Sex Differences in Facial Encoding of PainDocument14 pagesSex Differences in Facial Encoding of PainUmmu SolihahNo ratings yet
- Joels Copy of Final Paper Organization and Heading 2020Document17 pagesJoels Copy of Final Paper Organization and Heading 2020api-613093463No ratings yet
- Kevin Chen and Joseph J. Marbach - External Qigong Therapy For Chronic Orofacial Pain: A Letter To The EditorDocument5 pagesKevin Chen and Joseph J. Marbach - External Qigong Therapy For Chronic Orofacial Pain: A Letter To The EditorSonyRedNo ratings yet
- Pain and Gender Differences A Clinical ApproachDocument6 pagesPain and Gender Differences A Clinical ApproachMarianaNo ratings yet
- Distress With Medication Side Effects Among Persons With Severe Mental IllnessDocument9 pagesDistress With Medication Side Effects Among Persons With Severe Mental IllnessMaya Putri HaryantiNo ratings yet
- Women and The Experience of Pain and Opioid Use Disorder: A Literature-Based CommentaryDocument7 pagesWomen and The Experience of Pain and Opioid Use Disorder: A Literature-Based CommentarySUPHAWICH KHOIKAEWNo ratings yet
- Written Assigment-Pérez AndreaDocument6 pagesWritten Assigment-Pérez AndreaMaia TussieNo ratings yet
- Ache and MelancholyDocument30 pagesAche and MelancholyalinaferdohlebNo ratings yet
- 01 Ajp 0000210912 95664 53Document8 pages01 Ajp 0000210912 95664 53HEMACHANDRAN GNo ratings yet
- Testing A Theory of Chronic PainDocument13 pagesTesting A Theory of Chronic PainYuri Fiallos HernándezNo ratings yet
- None 2Document9 pagesNone 2Alfina RahmiNo ratings yet
- Artigo 2Document15 pagesArtigo 2Deise ArnasNo ratings yet
- Title: Depression, Pain and Physical Function in Patients With Osteoarthritis of The KneeDocument16 pagesTitle: Depression, Pain and Physical Function in Patients With Osteoarthritis of The Kneemohamad safiiNo ratings yet
- Association Between Severity of Pain, Perceived Stress and Vagally-Mediated Heart Rate Variability in Women With EndometriosisDocument11 pagesAssociation Between Severity of Pain, Perceived Stress and Vagally-Mediated Heart Rate Variability in Women With EndometriosisGerard Arbiol LópezNo ratings yet
- Freedom from Pain: Discover Your Body's Power to Overcome Physical PainFrom EverandFreedom from Pain: Discover Your Body's Power to Overcome Physical PainRating: 4.5 out of 5 stars4.5/5 (2)
- Nursing and Reflexology ResearchDocument39 pagesNursing and Reflexology ResearchJacqueline FerdinandNo ratings yet
- Testing A Theory of Chronic PainDocument13 pagesTesting A Theory of Chronic PainYuli FaiqoturrohmahNo ratings yet
- Pain and Pain Management in Elders With Knee Osteoarthritis in ChinaDocument10 pagesPain and Pain Management in Elders With Knee Osteoarthritis in ChinaSyarief NurseNo ratings yet
- Efektifitas Terapi Massage Dengan Terapi Mandi Air Hangat TerhadapDocument8 pagesEfektifitas Terapi Massage Dengan Terapi Mandi Air Hangat TerhadapAlfi Rohmatus SholihahNo ratings yet
- Quality of Life and Sexual Function of Women Affected by Endometriosis Associated Pelvic Pain When Treated With DienogestDocument8 pagesQuality of Life and Sexual Function of Women Affected by Endometriosis Associated Pelvic Pain When Treated With Dienogestliuyimin20100201No ratings yet
- Genital Pain and Sexual Functioning: Effects On Sexual Experience, Psychological Health, and Quality of LifeDocument13 pagesGenital Pain and Sexual Functioning: Effects On Sexual Experience, Psychological Health, and Quality of LifeSexologia Del OesteNo ratings yet
- DR Faisal Hayat FinalDocument11 pagesDR Faisal Hayat FinalbabuhaiderkhanNo ratings yet
- Running Head: Pain in The Older Adult 1Document10 pagesRunning Head: Pain in The Older Adult 1api-272656243No ratings yet
- Ca Mammae 1Document7 pagesCa Mammae 1Vera El Sammah SiagianNo ratings yet
- Effortless Pain Relief: A Guide to Self-Healing from Chronic PainFrom EverandEffortless Pain Relief: A Guide to Self-Healing from Chronic PainRating: 4.5 out of 5 stars4.5/5 (7)
- BMC Musculoskeletal Disorders: Fatigue in Osteoarthritis: A Qualitative StudyDocument8 pagesBMC Musculoskeletal Disorders: Fatigue in Osteoarthritis: A Qualitative StudyElvis Ponce AbarcaNo ratings yet
- Sex Differences in Insomnia: From Epidemiology and Etiology To InterventionDocument12 pagesSex Differences in Insomnia: From Epidemiology and Etiology To InterventionYudha HudayaNo ratings yet
- Fibromyalgia A Clinical ReviewDocument9 pagesFibromyalgia A Clinical ReviewastrogliaNo ratings yet
- Jurnal Mood and ImpressionDocument6 pagesJurnal Mood and ImpressionSinta HadriantiNo ratings yet
- Aldwin Park 2004 Coping and Physical Health OutcomesDocument6 pagesAldwin Park 2004 Coping and Physical Health OutcomespanospanNo ratings yet
- Bicket 2015Document14 pagesBicket 2015Giancarlo PalaciosNo ratings yet
- Research Paper Final Draft - Ali WeekleyDocument12 pagesResearch Paper Final Draft - Ali Weekleyapi-559220255No ratings yet
- Kaptein-Common-Sense Model-OsteoarthritisDocument9 pagesKaptein-Common-Sense Model-OsteoarthritisZyania MelchyNo ratings yet
- Altered Pain Sensitivity in Elderly Women With Chronic Neck PainDocument9 pagesAltered Pain Sensitivity in Elderly Women With Chronic Neck PainJhonny GradizNo ratings yet
- 6.ratial Gender Prevelnce PainDocument11 pages6.ratial Gender Prevelnce PainRiantiara PutrizaNo ratings yet
- Poor Sleep Quality Is Strongly Associated With Subsequent Pain Intensity in Patients With Acute Low Back PainDocument7 pagesPoor Sleep Quality Is Strongly Associated With Subsequent Pain Intensity in Patients With Acute Low Back Painapi-243703329No ratings yet
- Orofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelDocument27 pagesOrofacial Musculoskeletal Pain. An Evidence-Based Bio-Psycho-Social Matrix ModelAMBAR JOSEFA ALEJANDRA MORAGA VALENZUELANo ratings yet
- The Pain Anxiety Symptoms Scale - Development and Validation of A Scale To Measure Fear of PainDocument7 pagesThe Pain Anxiety Symptoms Scale - Development and Validation of A Scale To Measure Fear of Painapi-291366747No ratings yet
- Pain Management in Occupational Health: A Guide For Non-Narcotic Pain ReliefDocument7 pagesPain Management in Occupational Health: A Guide For Non-Narcotic Pain ReliefHaryaman JustisiaNo ratings yet
- Chronic Pain DissertationDocument7 pagesChronic Pain DissertationColumbia100% (1)
- More Than Just Bad Sex - Sexual Dysfunction and Distress in Patients With EndometriosisDocument5 pagesMore Than Just Bad Sex - Sexual Dysfunction and Distress in Patients With EndometriosisRoxana DalioNo ratings yet
- Sleep IssuesDocument7 pagesSleep IssuesASHUTOSH GAURAVNo ratings yet
- Michelle - Proctor@corrections - Govt.nz Cochrane Menstrual Disorders and Subfertility GroupDocument21 pagesMichelle - Proctor@corrections - Govt.nz Cochrane Menstrual Disorders and Subfertility GroupnarkeeshNo ratings yet
- Psychiatry Research: Eva Naumann, Brunna Tuschen-Caf Fier, Ulrich Voderholzer, Jennifer SvaldiDocument7 pagesPsychiatry Research: Eva Naumann, Brunna Tuschen-Caf Fier, Ulrich Voderholzer, Jennifer SvaldiAlexandra ErbaşuNo ratings yet
- Happy People Live Longer: Subjective Well-Being Contributes To Health and LongevityDocument65 pagesHappy People Live Longer: Subjective Well-Being Contributes To Health and LongevityPuteri Nur TriyandiniNo ratings yet
- สัมนาาาDocument7 pagesสัมนาาาBook AmornwadeeNo ratings yet
- The Effects of Massage Therapy On SleepDocument5 pagesThe Effects of Massage Therapy On SleepraniNo ratings yet
- Hypnosis and RelaxationDocument6 pagesHypnosis and RelaxationIustin MargineanuNo ratings yet
- Resilience PainDocument15 pagesResilience PainSara Bote GonzálezNo ratings yet
- Career DecisionDocument16 pagesCareer DecisionRiyad AliNo ratings yet
- AIME Post-Test Questions 09 08Document5 pagesAIME Post-Test Questions 09 08Riyad AliNo ratings yet
- QuestionsDocument5 pagesQuestionsRiyad AliNo ratings yet
- Sample MCQsDocument6 pagesSample MCQsRiyad AliNo ratings yet
- Q. What Is The Affected Cranial Nerve ?Document46 pagesQ. What Is The Affected Cranial Nerve ?Riyad AliNo ratings yet
- Physiology and Psychology of Acute Pain FINALDocument34 pagesPhysiology and Psychology of Acute Pain FINALRiyad AliNo ratings yet
- M.Muazzam Sheriff Lecturer Microbiology & Immunology Ibn Sina National College For Medical StudiesDocument24 pagesM.Muazzam Sheriff Lecturer Microbiology & Immunology Ibn Sina National College For Medical StudiesRiyad AliNo ratings yet
- T Lut: MG/DL)Document9 pagesT Lut: MG/DL)Riyad AliNo ratings yet
- Nociception Neuropathic Inflammatory PainDocument1 pageNociception Neuropathic Inflammatory PainRiyad AliNo ratings yet
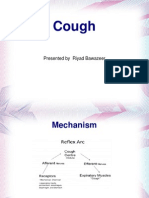
- Cough: Presented by Riyad BawazeerDocument4 pagesCough: Presented by Riyad BawazeerRiyad AliNo ratings yet
- PulseoximetryDocument2 pagesPulseoximetryRakshith NagarajaiahNo ratings yet
- A Robust Machine Learning Predictive Model For Maternal Health RiskDocument6 pagesA Robust Machine Learning Predictive Model For Maternal Health RiskjanvimalhotraofficialNo ratings yet
- Public Opinion On Idea of Digitalising Rural CommunityDocument11 pagesPublic Opinion On Idea of Digitalising Rural CommunityINSTITUTE OF LEGAL EDUCATIONNo ratings yet
- Export of SpicesDocument57 pagesExport of SpicesJunaid MultaniNo ratings yet
- AndmNotice 42 29 Posts Engl 070723 - 0Document3 pagesAndmNotice 42 29 Posts Engl 070723 - 0Awadhesh MalviyaNo ratings yet
- School Nutritional Status Record: Grade 7 - JoyDocument4 pagesSchool Nutritional Status Record: Grade 7 - JoySidNo ratings yet
- HSG 9 Hà Tĩnh 2021Document6 pagesHSG 9 Hà Tĩnh 2021Cachi100% (1)
- BA 89402175 001100 Innopack EN 00 PDFDocument293 pagesBA 89402175 001100 Innopack EN 00 PDFBruno GiffoniNo ratings yet
- Feeding Norms Poultry76Document14 pagesFeeding Norms Poultry76Ramesh BeniwalNo ratings yet
- Hearing Handicap Inventory For The Elderly (HHIE)Document5 pagesHearing Handicap Inventory For The Elderly (HHIE)Is GutiérrezNo ratings yet
- 10 - The Generics Act of 1988Document22 pages10 - The Generics Act of 1988rhydelNo ratings yet
- Quotes On StressDocument5 pagesQuotes On StressgretchhhNo ratings yet
- 1PE 4 Q3 Answer Sheet March 2024Document3 pages1PE 4 Q3 Answer Sheet March 2024Chid CabanesasNo ratings yet
- Free End SaddleDocument5 pagesFree End SaddleAdry AnnaNo ratings yet
- National Programme For Prevention and Control of FluorosisDocument49 pagesNational Programme For Prevention and Control of FluorosisveereshNo ratings yet
- Forensic MedicineDocument157 pagesForensic MedicineKNo ratings yet
- Flip Chart - My Health Is My Responsibility EnglishDocument28 pagesFlip Chart - My Health Is My Responsibility EnglishlivelinamiNo ratings yet
- Futuristic Nursing: - Sister Elizabeth DavisDocument14 pagesFuturistic Nursing: - Sister Elizabeth DavisPhebeDimple100% (2)
- R4 HealthfacilitiesDocument332 pagesR4 HealthfacilitiesCarl Joseph BarcenasNo ratings yet
- Poe Edgar Allan The Premature BurialDocument10 pagesPoe Edgar Allan The Premature BurialUntold TearNo ratings yet
- Electronic Care and Needs Scale eCANSDocument2 pagesElectronic Care and Needs Scale eCANSamanda wuNo ratings yet
- Aeon 4000 SDSDocument13 pagesAeon 4000 SDSmarcos luqueNo ratings yet
- INTEGRATED CASE STUDY: Cold Supply Chains and The COVID-19 VaccineDocument3 pagesINTEGRATED CASE STUDY: Cold Supply Chains and The COVID-19 VaccineKatia Katherine LUZON CURONo ratings yet
- Theories On Factors Affecting MotivationDocument24 pagesTheories On Factors Affecting Motivationmyra katrina mansan100% (5)
- Organ SystemsDocument2 pagesOrgan SystemsArnel LaspinasNo ratings yet
- Disaster Readiness Risk Reduction: Quarter 2-Module 13: DRR-related Laws and PoliciesDocument16 pagesDisaster Readiness Risk Reduction: Quarter 2-Module 13: DRR-related Laws and PoliciesUel Cabz LaquihonNo ratings yet
- Module 11 Rational Cloze Drilling ExercisesDocument9 pagesModule 11 Rational Cloze Drilling Exercisesperagas0% (1)
- Aquatics BrochureDocument24 pagesAquatics BrochurethuronNo ratings yet
- Stacey Waters CVDocument5 pagesStacey Waters CVapi-479651018No ratings yet
- How To Write A Case Report PDFDocument6 pagesHow To Write A Case Report PDFironNo ratings yet