You might also like
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- Insulin NewDocument41 pagesInsulin NewSheikNo ratings yet
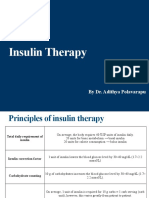
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- Basal Bolus Insulin Concept GuideDocument1 pageBasal Bolus Insulin Concept Guideocean329No ratings yet
- Insulin: Deciding How Much Insulin To TakeDocument12 pagesInsulin: Deciding How Much Insulin To Takeராபர்ட் ஆன்றோ ரெனி100% (1)
- Type 1 Diabetes Mellitus: TreatmentDocument25 pagesType 1 Diabetes Mellitus: TreatmentironNo ratings yet
- Insulin TypesDocument3 pagesInsulin TypesAbdullah A. ElgazarNo ratings yet
- Insulin & Oral Antidiabetic Drugs GuideDocument37 pagesInsulin & Oral Antidiabetic Drugs GuidePrithulNo ratings yet
- Standards of Care 2021 Figure 9.2Document2 pagesStandards of Care 2021 Figure 9.2Ariel GutierrezNo ratings yet
- Terapi Insulin-1Document46 pagesTerapi Insulin-1Yanti MoonNo ratings yet
- Fit-Diploma 3-2-2024Document57 pagesFit-Diploma 3-2-2024light tweenNo ratings yet
- Anti-Diabetic Drugs InsulinDocument26 pagesAnti-Diabetic Drugs Insulinwissam salimNo ratings yet
- DInsulin Types 1Document22 pagesDInsulin Types 1zahrabokerNo ratings yet
- Long Term DiabetesDocument68 pagesLong Term Diabetesnawaraj2044No ratings yet
- Adjusting Your Insulin DoseDocument3 pagesAdjusting Your Insulin DoseLib AsNo ratings yet
- Calculate The Dose of Diabetes MellitusDocument5 pagesCalculate The Dose of Diabetes MellitusOmar Nassir MoftahNo ratings yet
- Insulin Treatment in DiabetesDocument86 pagesInsulin Treatment in DiabetesAhsan Rauf100% (1)
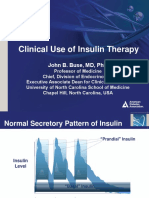
- Slide Clinical Use of Insulin Therapy (ADA)Document36 pagesSlide Clinical Use of Insulin Therapy (ADA)Dian SobaNo ratings yet
- Antidiabetic Agents GuideDocument19 pagesAntidiabetic Agents GuideJames SoeNo ratings yet
- InsulinDocument4 pagesInsulinHa Zizzle100% (1)
- Diabetes Part 1Document32 pagesDiabetes Part 1Zaid Al-KadhimiNo ratings yet
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- Insulin Therapy: Prof. Khalifa AbdallahDocument33 pagesInsulin Therapy: Prof. Khalifa AbdallahAhmed Adel MostafaNo ratings yet
- New Microsoft Word DocumentDocument2 pagesNew Microsoft Word Documenteslambasuony98No ratings yet
- Diabetes Study GuideDocument4 pagesDiabetes Study GuideNicole Brassington0% (1)
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument25 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateNeider 1111No ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Insulin History & Modality For Diabetic Patient: A. Makbul M. AmanDocument69 pagesInsulin History & Modality For Diabetic Patient: A. Makbul M. AmanRey Alwiwikh100% (1)
- General Principles of Insulin Therapy in Diabetes MellitusDocument12 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusRuban RichardNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Novolin and HumulinDocument3 pagesNovolin and HumulinChynnaNo ratings yet
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument20 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateabdulghaniNo ratings yet
- 4DM PresentationDocument57 pages4DM Presentationamal nassarNo ratings yet
- Insulin PharmacologyDocument1 pageInsulin PharmacologyzainabNo ratings yet
- Pharmacology of Diabetes Mellitus 2Document55 pagesPharmacology of Diabetes Mellitus 2maxamuud xuseenNo ratings yet
- The Essential Role of Insulin in Diabetes ManagementDocument9 pagesThe Essential Role of Insulin in Diabetes ManagementAbdul SamadNo ratings yet
- Effective Use of Insulin: PreviewDocument6 pagesEffective Use of Insulin: Previewprad1973No ratings yet
- Insulin PharmDocument21 pagesInsulin PharmMeredith Barb0% (1)
- Approsch To DM1Document4 pagesApprosch To DM1M MazloumNo ratings yet
- Adjunting Insuline DosisDocument5 pagesAdjunting Insuline DosisPaco TrooperNo ratings yet
- Pharmacology LectureDocument6 pagesPharmacology LectureAbdullahayad farouqNo ratings yet
- Diabetes Insulin InitiationDocument12 pagesDiabetes Insulin InitiationSatinder BhallaNo ratings yet
- Insulin Insulin Is A Hormone Central To Regulating Carbohydrate and Fat MetabolismDocument4 pagesInsulin Insulin Is A Hormone Central To Regulating Carbohydrate and Fat Metabolismmaeca101No ratings yet
- Insulin AspartDocument6 pagesInsulin AspartHutomo PrawirohardjoNo ratings yet
- Insulin, Oral Hypoglycaemic Agents, GlucagonDocument63 pagesInsulin, Oral Hypoglycaemic Agents, GlucagonBhavesh kunvarNo ratings yet
- Insulin TherapyDocument60 pagesInsulin Therapylight tweenNo ratings yet
- Insulin: T Ypes and Activit yDocument0 pagesInsulin: T Ypes and Activit yClara DohudeNo ratings yet
- Cases Illustrating Problems With Insulin Therapy For Diabetes MellitusDocument7 pagesCases Illustrating Problems With Insulin Therapy For Diabetes MellitusA.h.MuradNo ratings yet
- PANCREATIC HORMONES AND ANTIDIABETIC DRUGS: INSULIN AND SULFONYLUREASDocument5 pagesPANCREATIC HORMONES AND ANTIDIABETIC DRUGS: INSULIN AND SULFONYLUREASEric James ManuelNo ratings yet
- 2022 Insulin Calculations Cheat Sheet ARDocument4 pages2022 Insulin Calculations Cheat Sheet ARGulsama BabarNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Dietetik TerjemahDocument8 pagesDietetik TerjemahAsrori MuhofiNo ratings yet
- Readings (Insulin) - RetuyaDocument20 pagesReadings (Insulin) - RetuyaFionah RetuyaNo ratings yet
- Managing Diabetes with InsulinDocument47 pagesManaging Diabetes with InsulincedricNo ratings yet
- Endocrine CologyDocument124 pagesEndocrine CologyBehailu TejeNo ratings yet
- Hayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementDocument14 pagesHayatt Univesity College. Faculty of Medicine. Family Medicine. Mohamed Gassim Mohamed. Insulin ManagementMohammed GassimNo ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Mode of AssignmentDocument95 pagesMode of AssignmentQasim AliNo ratings yet
- Standardized Recipes - Doc2Document130 pagesStandardized Recipes - Doc2epic failNo ratings yet
- 1:21-cv-03674 Coomes, Williams, Slater & Tisbert vs. Centerra Group, LLCDocument16 pages1:21-cv-03674 Coomes, Williams, Slater & Tisbert vs. Centerra Group, LLCMichelle EdwardsNo ratings yet
- Intermolecular Forces Lesson PlanDocument34 pagesIntermolecular Forces Lesson Planapi-442754652No ratings yet
- Future Reference Craftsman Scroll Saw Serial and Model NumbersDocument22 pagesFuture Reference Craftsman Scroll Saw Serial and Model NumbersJL AlexanderNo ratings yet
- MWRC Policies & Procedures Manual 2020Document10 pagesMWRC Policies & Procedures Manual 2020Emma RyersonNo ratings yet
- Boq For Ifad Pump Project (Solar System With Drip & Microsprinkler Water Distribution)Document4 pagesBoq For Ifad Pump Project (Solar System With Drip & Microsprinkler Water Distribution)Mr. 420No ratings yet
- Plasma MachiningDocument14 pagesPlasma MachiningMayankNo ratings yet
- Diesel Engine Operation and DiagDocument76 pagesDiesel Engine Operation and DiagHafiezul Hassan100% (3)
- Format Bahasa Inggeris UPSR 2016 ENGLISH (013) Section ADocument33 pagesFormat Bahasa Inggeris UPSR 2016 ENGLISH (013) Section AVINOTININo ratings yet
- HANDOUT - Cell Transport Review WorksheetDocument4 pagesHANDOUT - Cell Transport Review WorksheetDenis Martinez100% (1)
- PT. Citilink Indonesia N P W P: 0 2 - 8 2 7 - 5 9 7 - 2 - 0 9 3 - 0 0 0 Jl. Raya Juanda Sawotratap Gedangan SidoarjoDocument2 pagesPT. Citilink Indonesia N P W P: 0 2 - 8 2 7 - 5 9 7 - 2 - 0 9 3 - 0 0 0 Jl. Raya Juanda Sawotratap Gedangan SidoarjoZemNo ratings yet
- Sip Annex 3 Gap Analysis Template EditedDocument5 pagesSip Annex 3 Gap Analysis Template EditedRiza GusteNo ratings yet
- Inverter Controlled Mig Welding-Machine YD-400GT3 Operating ManualDocument53 pagesInverter Controlled Mig Welding-Machine YD-400GT3 Operating ManualsunhuynhNo ratings yet
- 可汗语法48篇(明志教育推荐) PDFDocument163 pages可汗语法48篇(明志教育推荐) PDFtellmewhour100% (2)
- Fire Safety in Public BuildingDocument48 pagesFire Safety in Public BuildingSamirsinh ParmarNo ratings yet
- TYF Oxit: Ready-to-Use, High-Performance Ultra Low Viscous Secondary Refrigerants For Applications Down To - 50 °CDocument9 pagesTYF Oxit: Ready-to-Use, High-Performance Ultra Low Viscous Secondary Refrigerants For Applications Down To - 50 °Cmarcyel Oliveira WoliveiraNo ratings yet
- Midterm MMMDocument2 pagesMidterm MMMasdfghjkl zxcvbnmNo ratings yet
- NABARD Presentation On FPODocument14 pagesNABARD Presentation On FPOSomnath DasGupta71% (7)
- Inas Faiqah BT Mohd Helmi (An Infant Suing Through Her Father and Next Friend, Mohd Helmi Bin Abdul Aziz) V Kerajaan Malaysia & OrsDocument15 pagesInas Faiqah BT Mohd Helmi (An Infant Suing Through Her Father and Next Friend, Mohd Helmi Bin Abdul Aziz) V Kerajaan Malaysia & Orsshukri77No ratings yet
- 08 Ergonomics - 01Document35 pages08 Ergonomics - 01Cholan PillaiNo ratings yet
- Hazard Identification 2. Risk AssessmentDocument5 pagesHazard Identification 2. Risk AssessmentNoreen Syakireen Binti NormanNo ratings yet
- Plastipak PresentationDocument28 pagesPlastipak Presentationapi-608970005No ratings yet
- Audi A6 Allroad Model 2013 Brochure - 2012.08Document58 pagesAudi A6 Allroad Model 2013 Brochure - 2012.08Arkadiusz KNo ratings yet
- Stabilizers: Agusta A W139 Maintenance Course Training ManualDocument6 pagesStabilizers: Agusta A W139 Maintenance Course Training ManualNita PuteriNo ratings yet
- A300-600 Ammfx1 29 24 00 03 0Document5 pagesA300-600 Ammfx1 29 24 00 03 0Fahimeh HayatinasabNo ratings yet
- Exercise 5 - Journalizing TransactionsDocument10 pagesExercise 5 - Journalizing TransactionsMichael DiputadoNo ratings yet
- Chapter 1Document52 pagesChapter 1MD NAYM MIANo ratings yet
- Sub-Zero Icing Your Testicles For Increased Male Performance - MyBioHack Unlock Your Maximus PotentialDocument7 pagesSub-Zero Icing Your Testicles For Increased Male Performance - MyBioHack Unlock Your Maximus PotentialfortnitediscordbgweeNo ratings yet
- 25 Mechanical Engineering Interview Questions and Answers - Freshers, ExperiencedDocument7 pages25 Mechanical Engineering Interview Questions and Answers - Freshers, ExperiencedAnonymous RVO3O6zm0No ratings yet