You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Corrosion Mechanism Prevention Repair Measures of RCC StructureDocument217 pagesCorrosion Mechanism Prevention Repair Measures of RCC StructureAvinash Mandal100% (1)
- Evaluation of ToothpasteDocument8 pagesEvaluation of ToothpasteBINDUNo ratings yet
- Premenstrual Dysphoric Disorder: Evaluation, Pathophysiology and TreatmentDocument7 pagesPremenstrual Dysphoric Disorder: Evaluation, Pathophysiology and TreatmentBINDUNo ratings yet
- Topical GelDocument4 pagesTopical GelBINDUNo ratings yet
- Pain & Analgesics: DR - KumarasingamDocument22 pagesPain & Analgesics: DR - KumarasingamBINDUNo ratings yet
- Communication Strategies: #1 Strategy: Talk, Care and ConnectDocument29 pagesCommunication Strategies: #1 Strategy: Talk, Care and ConnectBINDUNo ratings yet
- Chemical Tests in PharmacognosyDocument30 pagesChemical Tests in PharmacognosyBINDU100% (9)
- Sanket GodeDocument2 pagesSanket GodeBINDUNo ratings yet
- Saurabh Updted CVDocument2 pagesSaurabh Updted CVBINDUNo ratings yet
- Formulation EvalutionDocument6 pagesFormulation EvalutionBINDUNo ratings yet
- AnalysisDocument14 pagesAnalysisBINDU100% (1)
- Saurabh Updted CVDocument2 pagesSaurabh Updted CVBINDUNo ratings yet
- 04 P064 34613Document14 pages04 P064 34613BINDUNo ratings yet
- All Stainless Steel Pressure Gauges With Bourdon TubeDocument2 pagesAll Stainless Steel Pressure Gauges With Bourdon TubetitiNo ratings yet
- Additive 510 m14Document5 pagesAdditive 510 m14MohsenNo ratings yet
- 1 4122Document1 page1 4122Zeeshan AnwarNo ratings yet
- Chapter 17 - Organic Chemistry PDFDocument18 pagesChapter 17 - Organic Chemistry PDFAarush SharmaNo ratings yet
- Khan 2014Document11 pagesKhan 2014Hidayat Jamalul INo ratings yet
- Ceramics and Its Importance: AbstractDocument3 pagesCeramics and Its Importance: AbstractPrabandari SyamNo ratings yet
- Thesis 2013 AlhutmanyDocument178 pagesThesis 2013 AlhutmanyMohammed Zahir Al-KilaniNo ratings yet
- Clasificación de Productos para El Cuidado de La PielDocument1 pageClasificación de Productos para El Cuidado de La PielPapaindoNo ratings yet
- 89145000ENDocument3 pages89145000ENAya HalimNo ratings yet
- TurboFP635 (Print)Document1 pageTurboFP635 (Print)triplegreenhandNo ratings yet
- FevicolDocument2 pagesFevicolSayli JadhavNo ratings yet
- Presentazione Avocado Oil AGG. 2023 - ENG RevDocument20 pagesPresentazione Avocado Oil AGG. 2023 - ENG RevAlpha ShilaNo ratings yet
- NDT 2 Mark Questions All Units PDFDocument11 pagesNDT 2 Mark Questions All Units PDFlingarajNo ratings yet
- A Molecular Approach ch16Document179 pagesA Molecular Approach ch16StephenNo ratings yet
- Jclepro D 23 19785Document17 pagesJclepro D 23 19785david.pinzonNo ratings yet
- Lab Report 2Document12 pagesLab Report 2Fatihah AlhataNo ratings yet
- Structural SteelDocument3 pagesStructural SteelNarendra PalandeNo ratings yet
- Exp 1 Chm510Document11 pagesExp 1 Chm510Nur Nadia Syahira100% (1)
- Solid State FermentationDocument19 pagesSolid State FermentationFaaye ZzaaNo ratings yet
- 547 PDFDocument389 pages547 PDFMohammed sabatinNo ratings yet
- A Review On Stability Indicating HPLC Method DevelopmentDocument19 pagesA Review On Stability Indicating HPLC Method DevelopmentppiccoliniNo ratings yet
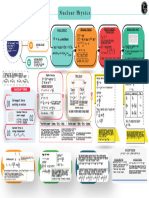
- Nuclear Physics - Mind Map - Lakshya NEET 2024Document1 pageNuclear Physics - Mind Map - Lakshya NEET 2024aanyakaurchonaNo ratings yet
- Simulation Thermal Behaviour of Concrete by FEA A STAR Review (ICT Newsletter)Document1 pageSimulation Thermal Behaviour of Concrete by FEA A STAR Review (ICT Newsletter)s80johnnyNo ratings yet
- High Pressure Processing of FoodsDocument19 pagesHigh Pressure Processing of FoodsJagan DeepNo ratings yet
- C5240HP Technical Data Ver.1.1Document8 pagesC5240HP Technical Data Ver.1.1顏健軒No ratings yet
- Alkohol...Document47 pagesAlkohol...R.Afr26 0403No ratings yet
- Soil Mech and Foundation by XYZDocument73 pagesSoil Mech and Foundation by XYZParamveer SharmaNo ratings yet
- MSDS Fe (NO3) 3 PDFDocument4 pagesMSDS Fe (NO3) 3 PDFAngga Pamilu PutraNo ratings yet
- Primitive Unit Cells - MSEstudentComDocument20 pagesPrimitive Unit Cells - MSEstudentComJuano Valls FerrerNo ratings yet