You might also like
- Hiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Document55 pagesHiv Treatment: IC2 Haemato-Lymphoid and Tropical Medicine HLTM Dr. Eoghan de Barra 2014Faiq Syukri Bin SaparudinNo ratings yet
- Erica Stewart Belhaven FileDocument33 pagesErica Stewart Belhaven Filethe kingfishNo ratings yet
- The Virus Misconception Part 1 Measles As An Example by DR Stefan LankaDocument14 pagesThe Virus Misconception Part 1 Measles As An Example by DR Stefan Lankatrixstar108087100% (2)
- Is HIV The Biggest Mistake of XXcenturyDocument14 pagesIs HIV The Biggest Mistake of XXcenturyMartini100% (1)
- Teaching No Greater CallingDocument256 pagesTeaching No Greater CallinggabrielpoulsonNo ratings yet
- Kicking Off: Getting Started in The Christian LifeDocument59 pagesKicking Off: Getting Started in The Christian Lifelpac9387No ratings yet
- Is PPT CompleteDocument456 pagesIs PPT CompleteCelso Rodil IIINo ratings yet
- HIV NutritionDocument7 pagesHIV NutritionBrian Hunter Levins Jr.No ratings yet
- Hiv Infection and AidsDocument51 pagesHiv Infection and Aidspokhara gharipatanNo ratings yet
- Blood and Immunity Study GuideDocument4 pagesBlood and Immunity Study GuideKimberly PollyNo ratings yet
- 01 - General Feature of VirusDocument2 pages01 - General Feature of VirusSajid Ali100% (1)
- Tuberculosis: Cause and TransmissionDocument6 pagesTuberculosis: Cause and TransmissionAnkit SharmaNo ratings yet
- Case 10 Hiv-AidsDocument47 pagesCase 10 Hiv-AidsErikah Eirah BeloriaNo ratings yet
- Atypical BacteriaDocument19 pagesAtypical BacteriaHabibur RahamanNo ratings yet
- 6 Inhibiting The Growth of Pathogens in VivoDocument27 pages6 Inhibiting The Growth of Pathogens in VivoAinaB ManaloNo ratings yet
- PROF SURYANI-Medical Nutrition Therapy NeuroDocument52 pagesPROF SURYANI-Medical Nutrition Therapy NeuroAsriNo ratings yet
- Hiv PPDocument37 pagesHiv PPJitendra YadavNo ratings yet
- General Characteristics of Viruses PDFDocument2 pagesGeneral Characteristics of Viruses PDFabdulNo ratings yet
- Oral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNDocument74 pagesOral Fecal Route Diseases Oral Fecal Route Diseases: Afroz Lakhani RN, BSCNafrozlakhaniNo ratings yet
- Basic ImmunologyDocument57 pagesBasic ImmunologyRonalyn UgatNo ratings yet
- Tuberculosis EssayDocument16 pagesTuberculosis EssayDineswari RemyndranNo ratings yet
- Infectious DiseasesDocument144 pagesInfectious DiseasesMd.Mahmudul HasanNo ratings yet
- Virologists FraudstersDocument12 pagesVirologists FraudstersMalden Mldn100% (1)
- Scrub TyphusDocument2 pagesScrub TyphusitsankurzNo ratings yet
- Vulvovaginal Candidiasis and Bacterial VaginosisDocument16 pagesVulvovaginal Candidiasis and Bacterial VaginosisAdnanda Maulan100% (1)
- StdsDocument14 pagesStdsJumar Divinagracia DimpasNo ratings yet
- Specific Host Defenses: The Immune ResponseDocument54 pagesSpecific Host Defenses: The Immune Responseadyaly44No ratings yet
- Introduction To Immunology, Science of ImmunityDocument80 pagesIntroduction To Immunology, Science of Immunitytummalapalli venkateswara raoNo ratings yet
- 01 - General Structure and Classification of Viruses1Document38 pages01 - General Structure and Classification of Viruses1Rahul Kumar100% (1)
- Cytokines & Their ActionsDocument59 pagesCytokines & Their ActionsSharanabasappa DurgNo ratings yet
- SPIROCHETESDocument11 pagesSPIROCHETESShujat Razaq100% (1)
- Overview of The Immune System 2020Document31 pagesOverview of The Immune System 2020mehakNo ratings yet
- Are Viruses Living or Non-Living Organisms?Document8 pagesAre Viruses Living or Non-Living Organisms?Sydney Cloyce NagalNo ratings yet
- Components of The Immune SystemDocument8 pagesComponents of The Immune Systemبراءة أحمد السلاماتNo ratings yet
- BiologyDocument27 pagesBiologyAnand GNo ratings yet
- Care Plan For HIVDocument20 pagesCare Plan For HIVlanguha NgatiNo ratings yet
- Chapter 12 Drugs, Microbes, The Elements of Chemotherapy: Building Your KnowledgeDocument12 pagesChapter 12 Drugs, Microbes, The Elements of Chemotherapy: Building Your Knowledgemalenya1100% (1)
- Women and HIVDocument217 pagesWomen and HIVMuhammad Ricky RamadhianNo ratings yet
- Principles and Practice of AsepsisDocument24 pagesPrinciples and Practice of AsepsisMuhammad AdamNo ratings yet
- Pertusis TreatmentDocument20 pagesPertusis TreatmentJaipratap SinghNo ratings yet
- HowtoWriteaGreatStatementofPurposePowerPoint April2010Document22 pagesHowtoWriteaGreatStatementofPurposePowerPoint April2010George PailyNo ratings yet
- Medical ParasitologyDocument53 pagesMedical ParasitologyCandilicious10No ratings yet
- Alteration in Immune ResponseDocument29 pagesAlteration in Immune ResponsePachita AlexandruNo ratings yet
- HIV and AIDS - PDF 2Document26 pagesHIV and AIDS - PDF 2Cheska JunturaNo ratings yet
- Immune SystemDocument11 pagesImmune SystemMar'atus SilmiahNo ratings yet
- Antibiotics FruitDocument5 pagesAntibiotics FruitxprakashNo ratings yet
- Mikrobiologi Virus ArthropodeDocument55 pagesMikrobiologi Virus Arthropodeakun scribNo ratings yet
- Virology Techniques: Chapter 5 - Lesson 4Document8 pagesVirology Techniques: Chapter 5 - Lesson 4Ramling PatrakarNo ratings yet
- Immunoparasitology and Fungal ImmunityDocument31 pagesImmunoparasitology and Fungal ImmunityShakti PatelNo ratings yet
- Bacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityDocument20 pagesBacterial Toxins: Yogi Khoirul Abror Departement of Immunology Postgraduate Programme Airlangga UniversityYogiabrorNo ratings yet
- Management of Urinary Tract Infections in PregnancyDocument26 pagesManagement of Urinary Tract Infections in PregnancySylvia WijayaNo ratings yet
- Bordetella Pertussis and Whooping CoughDocument22 pagesBordetella Pertussis and Whooping CoughDian TikaNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- Antigens & Antigen Presentation: Prof Anura WeerasingheDocument21 pagesAntigens & Antigen Presentation: Prof Anura Weerasinghesiva100% (1)
- ZIKA VIRUS INFECTION Emerging Public Health ConcernDocument36 pagesZIKA VIRUS INFECTION Emerging Public Health Concerntummalapalli venkateswara rao100% (1)
- History of ImmunologyDocument6 pagesHistory of ImmunologyKitt KittNo ratings yet
- Health, Stress, and CopingDocument43 pagesHealth, Stress, and CopingKar Gayee100% (1)
- Complementary/ Alternative MedicineDocument61 pagesComplementary/ Alternative MedicineKeith OmwoyoNo ratings yet
- 2 Pathophysiology of HIVDocument8 pages2 Pathophysiology of HIVRaga ManduaruNo ratings yet
- 2 Pa Tho Physiology of HIVDocument8 pages2 Pa Tho Physiology of HIVLeepin TanNo ratings yet
- 2998-Article Text-8874-1-10-20190629Document3 pages2998-Article Text-8874-1-10-20190629Indra DhootNo ratings yet
- D Pharma 1st PCDocument46 pagesD Pharma 1st PCIndra DhootNo ratings yet
- Pharmaceutics Lab Manual 1Document18 pagesPharmaceutics Lab Manual 1Indra Dhoot100% (1)
- Hap 2Document1 pageHap 2Indra DhootNo ratings yet
- Updated Enclosure-2 and 3Document2 pagesUpdated Enclosure-2 and 3Indra DhootNo ratings yet
- Gene TherapyDocument30 pagesGene TherapyIndra DhootNo ratings yet
- For Pharm.D:: WWW - Pci.nic - inDocument2 pagesFor Pharm.D:: WWW - Pci.nic - inBhanu K PrakashNo ratings yet
- Alzimer DiseaseDocument58 pagesAlzimer DiseaseIndra Dhoot100% (1)
- For Pharm.D:: WWW - Pci.nic - inDocument2 pagesFor Pharm.D:: WWW - Pci.nic - inBhanu K PrakashNo ratings yet
- The 10 Most Famousfilipino Artists and Their MasterworksDocument3 pagesThe 10 Most Famousfilipino Artists and Their MasterworksGina MagtibayNo ratings yet
- Sap Ewm OverviewDocument11 pagesSap Ewm OverviewsachinNo ratings yet
- Climbing FormworkDocument4 pagesClimbing FormworkAshwin B S RaoNo ratings yet
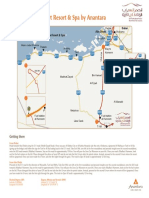
- Qasr Al Sarab Desert Resort Location Map June2012Document1 pageQasr Al Sarab Desert Resort Location Map June2012Anant GârgNo ratings yet
- Carrefour-SA Shopping Center TurkeyDocument2 pagesCarrefour-SA Shopping Center TurkeyVineet JogalekarNo ratings yet
- Lima Indiana Oil FieldDocument32 pagesLima Indiana Oil FieldCHARLES PATULAYNo ratings yet
- Designing and Building A Computer TableDocument9 pagesDesigning and Building A Computer Tablemaster_codersNo ratings yet
- Ecall Vs NG EcallDocument6 pagesEcall Vs NG EcallTrần Văn DũngNo ratings yet
- Worksheet - 143760187HS-II, TUTORIAL ON CH-5Document14 pagesWorksheet - 143760187HS-II, TUTORIAL ON CH-5A MusaverNo ratings yet
- Chapter 7 - Stress - TransformationsDocument21 pagesChapter 7 - Stress - TransformationsroselleNo ratings yet
- Asteroids Prospective EnergyDocument710 pagesAsteroids Prospective EnergySlavica Otovic100% (1)
- F24 60manual (New)Document14 pagesF24 60manual (New)Robert CumpaNo ratings yet
- FebvreDocument449 pagesFebvreIan Pereira AlvesNo ratings yet
- 1n5711 RF Detector Diode 70v PIV DatasheetDocument3 pages1n5711 RF Detector Diode 70v PIV DatasheetgordslaterNo ratings yet
- Contoh CV / Daftar Riwayat HidupDocument2 pagesContoh CV / Daftar Riwayat HiduprusmansyahNo ratings yet
- W0L0XCF0866101640 (2006 Opel Corsa) PDFDocument7 pagesW0L0XCF0866101640 (2006 Opel Corsa) PDFgianyNo ratings yet
- Airport Security Post 9-11Document7 pagesAirport Security Post 9-11lewisNo ratings yet
- List of Fatigue Standards and Fracture Standards Developed by ASTM & ISODocument3 pagesList of Fatigue Standards and Fracture Standards Developed by ASTM & ISOSatrio Aditomo100% (1)
- CS402 Mcqs MidTerm by Vu Topper RMDocument50 pagesCS402 Mcqs MidTerm by Vu Topper RMM. KhizarNo ratings yet
- Pellicon 2 Validation Guide PDFDocument45 pagesPellicon 2 Validation Guide PDFtakwahs12135No ratings yet
- Minimalist KWL Graphic OrganizerDocument2 pagesMinimalist KWL Graphic OrganizerIrish Nicole AlanoNo ratings yet
- Clinical Biomechanics: Leigh W. Marshall, Stuart M. McgillDocument4 pagesClinical Biomechanics: Leigh W. Marshall, Stuart M. McgillMichael JunNo ratings yet
- Region 1 - Concreting Works Materials Prices - PHILCON PRICESDocument9 pagesRegion 1 - Concreting Works Materials Prices - PHILCON PRICESMark Gregory RimandoNo ratings yet
- T.A.T.U. - Waste Management - Digital BookletDocument14 pagesT.A.T.U. - Waste Management - Digital BookletMarieBLNo ratings yet
- Electronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMDocument2 pagesElectronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMNesha Siva Shanmugam ShavannahNo ratings yet
- V. Jovicic and M. R. Coop1997 - Stiffness, Coarse Grained Soils, Small StrainsDocument17 pagesV. Jovicic and M. R. Coop1997 - Stiffness, Coarse Grained Soils, Small StrainsxiangyugeotechNo ratings yet
- G10Mapeh Exam First QuaterDocument8 pagesG10Mapeh Exam First QuaterJonas LamcisNo ratings yet
- Raneem AlbazazDocument33 pagesRaneem AlbazazGordana PuzovicNo ratings yet
- Test09 Eoc Algebra2 ReducedDocument33 pagesTest09 Eoc Algebra2 ReducedkristymadimikeNo ratings yet
- Discrete Wavelet TransformDocument10 pagesDiscrete Wavelet TransformVigneshInfotechNo ratings yet