You might also like
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Differential Diagnosis of NICODocument13 pagesDifferential Diagnosis of NICOscribdmikaelNo ratings yet
- 15.Trigeminal neuralgiaDocument25 pages15.Trigeminal neuralgiaBhakti WashilkarNo ratings yet
- Trigeminal Neuralgia: Presented By: DR Abdullah Mumtaz BDS Roll# 03Document25 pagesTrigeminal Neuralgia: Presented By: DR Abdullah Mumtaz BDS Roll# 03Chaudhry Abdullah DeuNo ratings yet
- Acc 61 - Supp2 96Document7 pagesAcc 61 - Supp2 96intermediosamberesNo ratings yet
- Trigeminal NeuralgiaDocument6 pagesTrigeminal NeuralgiaputrisarahNo ratings yet
- NerualgiaDocument7 pagesNerualgiaKabirNo ratings yet
- Wilhour-Nahas2018 Article The NeuralgiasDocument8 pagesWilhour-Nahas2018 Article The NeuralgiasCamilo Benavides BurbanoNo ratings yet
- Mendoza Outline of DiseasesDocument28 pagesMendoza Outline of DiseasesAleks MendozaNo ratings yet
- Trigeminal Neuralgia: FJ Dowd, Creighton University School of Medicine, Omaha, NE, USADocument5 pagesTrigeminal Neuralgia: FJ Dowd, Creighton University School of Medicine, Omaha, NE, USAWalter Espinoza CiertoNo ratings yet
- Primary Headache Secondary HeadacheDocument5 pagesPrimary Headache Secondary HeadacheYolanda Dwi OktaviyaniNo ratings yet
- 7vol6issue5p28-32 20200918050408Document5 pages7vol6issue5p28-32 20200918050408SkAliHassanNo ratings yet
- Trigeminal NeuralgiaDocument6 pagesTrigeminal NeuralgiamimirkuNo ratings yet
- What Is Trigeminal NeuralgiaDocument3 pagesWhat Is Trigeminal NeuralgiakewpietheresaNo ratings yet
- Lapsus Ablasi Radiofrekuensi Pada Neuralgia Trigeminal Dengan Panduan FluoroskopiDocument8 pagesLapsus Ablasi Radiofrekuensi Pada Neuralgia Trigeminal Dengan Panduan FluoroskopivalenciaNo ratings yet
- Otolaryngologist Guide to Diagnosing Common Headaches and Facial PainDocument15 pagesOtolaryngologist Guide to Diagnosing Common Headaches and Facial PainYuniParaditaDjunaidiNo ratings yet
- Overview of Craniofacial Pain - UpToDateDocument24 pagesOverview of Craniofacial Pain - UpToDateNana ShkodinaNo ratings yet
- Headache+Medicine,+v 3,+n 2,+p 76-87,+apr MayJun +2012Document12 pagesHeadache+Medicine,+v 3,+n 2,+p 76-87,+apr MayJun +2012dvdbergamascoNo ratings yet
- Trigeminal NeuralgiaDocument18 pagesTrigeminal NeuralgiaKaran KohliNo ratings yet
- Pharmacotherapeuticsiii Assignment-Ii - Neuralgias: By-Shaheestha Tabasum Roll No: 18111T0014 Pharmd 4thyrDocument439 pagesPharmacotherapeuticsiii Assignment-Ii - Neuralgias: By-Shaheestha Tabasum Roll No: 18111T0014 Pharmd 4thyrtabasum shahhNo ratings yet
- Trigeminal NeuralgiaDocument54 pagesTrigeminal NeuralgiaSarah Khan100% (1)
- Trigeminal NeuralgiaDocument7 pagesTrigeminal NeuralgiaEricsonMitraNo ratings yet
- Trigeminal NeuralgiaDocument72 pagesTrigeminal NeuralgiaCocoMathewNo ratings yet
- Trigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalDocument57 pagesTrigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalAmy Rose EugenioNo ratings yet
- Trigeminal Neuralgia - UpToDateDocument28 pagesTrigeminal Neuralgia - UpToDateCalvin Van ChenNo ratings yet
- Treatment For Central Pain Syndrome 2007Document0 pagesTreatment For Central Pain Syndrome 2007Merari Lugo OcañaNo ratings yet
- Trigeminal NeuralgiaDocument35 pagesTrigeminal NeuralgiaMahad abuukarNo ratings yet
- Orofacial Pain (OFP) : Oral MedicineDocument22 pagesOrofacial Pain (OFP) : Oral Medicineآيات محمد تعبان هليلNo ratings yet
- Facial Pain Types and Causes: A Guide for DentistsDocument7 pagesFacial Pain Types and Causes: A Guide for DentistsNada BrassnNo ratings yet
- A New Theory and Case Report - David B. Miller D.D.S PDFDocument11 pagesA New Theory and Case Report - David B. Miller D.D.S PDFdrgayen60420% (1)
- Pemicu 1: Blok Sistem Saraf Dan KejiwaanDocument50 pagesPemicu 1: Blok Sistem Saraf Dan KejiwaancecilliacynthiaNo ratings yet
- Orofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsDocument49 pagesOrofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsmishaNo ratings yet
- Glossopharyngeal NeuralgiaDocument6 pagesGlossopharyngeal Neuralgiaflorin jescuNo ratings yet
- Atlas of Uncommon Pain Syndromes. Expert Consult - Online and PrintDocument374 pagesAtlas of Uncommon Pain Syndromes. Expert Consult - Online and PrintLorena Fernandez100% (2)
- Neuropathies: Mrs. Keerthana.B Assistant Professor MSN, PSG ConDocument65 pagesNeuropathies: Mrs. Keerthana.B Assistant Professor MSN, PSG ConKeerthana BNo ratings yet
- TrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569Document9 pagesTrigeminalNeuralgiaPracticeEssentials, Background, Anatomy 1700148132569esthersilingi12No ratings yet
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaPao JeyNo ratings yet
- Tolosa-Hunt Syndrome: EpidemiologyDocument3 pagesTolosa-Hunt Syndrome: EpidemiologyRiris SihotangNo ratings yet
- AN C F P: EW Lassification For Acial AINDocument4 pagesAN C F P: EW Lassification For Acial AINAkmal Niam FirdausiNo ratings yet
- The Neuralgias Diagnosis and Management Curr Neurol Neurosci Rep 2014Document8 pagesThe Neuralgias Diagnosis and Management Curr Neurol Neurosci Rep 2014Fernando BravoNo ratings yet
- Trigeminal Neuralgia in a Young Female Patient with V1 InvolvementDocument19 pagesTrigeminal Neuralgia in a Young Female Patient with V1 Involvement6ixSideCreate MNo ratings yet
- Glossopharyngeal NeuralgiaDocument3 pagesGlossopharyngeal NeuralgiaNegin HekmatjooNo ratings yet
- Facial Pain PDFDocument4 pagesFacial Pain PDFSuprit SnNo ratings yet
- Neuropathic Pain of Postherpetic Neuralgia: All Rights R Eserved. ReprDocument0 pagesNeuropathic Pain of Postherpetic Neuralgia: All Rights R Eserved. ReprMarliani AfriastutiNo ratings yet
- Trigeminal Neuralgia: Intense, Shooting, Stabbing Pain That Is Similar To Electric ShocksDocument5 pagesTrigeminal Neuralgia: Intense, Shooting, Stabbing Pain That Is Similar To Electric ShocksDepiinaNo ratings yet
- Trigeminal Neuralgia Recent Approach in ClassificaDocument9 pagesTrigeminal Neuralgia Recent Approach in ClassificaFKUPR 2017No ratings yet
- Allam Anthony K Trigeminal NeuralgiaDocument15 pagesAllam Anthony K Trigeminal NeuralgiaAnonymous tG35SYROzENo ratings yet
- Clinical Aspects of Trigeminal Neuralgia: A Systematic ReviewDocument5 pagesClinical Aspects of Trigeminal Neuralgia: A Systematic ReviewPratik ParikhNo ratings yet
- Q1.Flaccid Paresis: Diagnostical VariantsDocument47 pagesQ1.Flaccid Paresis: Diagnostical VariantsNelson OduorNo ratings yet
- Trigeminal Autonomic CephalgiasDocument15 pagesTrigeminal Autonomic Cephalgiasheni taridaNo ratings yet
- Familial Trigeminal Neuralgia (Case Report) : Nicolae Cârciumaru, Irene Damian Constanta, RomaniaDocument4 pagesFamilial Trigeminal Neuralgia (Case Report) : Nicolae Cârciumaru, Irene Damian Constanta, RomaniaGarryNo ratings yet
- Facial Pain Diagnosis GuideDocument11 pagesFacial Pain Diagnosis GuidesaswepakNo ratings yet
- Differentiating Trigeminal Neuropathy From Trigeminal NeuralgiaDocument11 pagesDifferentiating Trigeminal Neuropathy From Trigeminal NeuralgiaGarryNo ratings yet
- Neurophatic PainDocument4 pagesNeurophatic PainicoanamareNo ratings yet
- A Case of Occipital NeuralgiaDocument20 pagesA Case of Occipital NeuralgiaLakNo ratings yet
- Understanding Trigeminal Neuralgia and Atypical Facial PainDocument41 pagesUnderstanding Trigeminal Neuralgia and Atypical Facial PainEuOmi Alsheikh100% (1)
- 2008 Trigeminal NeuralgiaDocument6 pages2008 Trigeminal NeuralgiaApril Rose Airoso - AramburoNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Neurology Multiple Choice Questions With Explanations: Volume IIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIRating: 5 out of 5 stars5/5 (2)
- Flare-Ups in Endodontics - A Review: Priyanka.S.R, DR - VeronicaDocument6 pagesFlare-Ups in Endodontics - A Review: Priyanka.S.R, DR - VeronicaHadil AltilbaniNo ratings yet
- Pain and FL Are-Up After Endodontic Treatment Procedures: ReviewDocument6 pagesPain and FL Are-Up After Endodontic Treatment Procedures: ReviewGin Gin GustianaNo ratings yet
- Disassembly Re TX Part 22004Document4 pagesDisassembly Re TX Part 22004Hadil AltilbaniNo ratings yet
- Endodontics Eng SMF PDFDocument32 pagesEndodontics Eng SMF PDFIulia CiobanuNo ratings yet
- Guidelines for Surgical Endodontic ProceduresDocument11 pagesGuidelines for Surgical Endodontic ProceduresgrzeniouNo ratings yet
- Masticatory Force Measurement in Natural Dentition: Himmlova@seznam - CZ WWW - Vus.czDocument1 pageMasticatory Force Measurement in Natural Dentition: Himmlova@seznam - CZ WWW - Vus.czHadil AltilbaniNo ratings yet
- Governments Should Spend Money On Railways Rather Than RoadsDocument2 pagesGovernments Should Spend Money On Railways Rather Than RoadsHadil Altilbani100% (2)
- MusicDocument2 pagesMusicHadil AltilbaniNo ratings yet
- Writeshortnoteson 140422174941 Phpapp02 PDFDocument1 pageWriteshortnoteson 140422174941 Phpapp02 PDFHadil Altilbani100% (1)
- English - How To Prepare For IELTS PDFDocument7 pagesEnglish - How To Prepare For IELTS PDFmrcpianNo ratings yet
- Single Visit Versus Multiple Visit Root Canal TherapyDocument8 pagesSingle Visit Versus Multiple Visit Root Canal TherapyHadil AltilbaniNo ratings yet
- Sodium Hypochlorite and Its Use An Endodontic IrrigantDocument7 pagesSodium Hypochlorite and Its Use An Endodontic IrrigantHadil AltilbaniNo ratings yet
- Sodium Hypochlorite inDocument13 pagesSodium Hypochlorite inDr.O.R.GANESAMURTHINo ratings yet
- Economic Progress Is Their Most ImportantDocument1 pageEconomic Progress Is Their Most ImportantHadil AltilbaniNo ratings yet
- Governments should measure progress beyond just economicsDocument1 pageGovernments should measure progress beyond just economicsHadil AltilbaniNo ratings yet
- Ielts Task 2 6 Sample EssaysDocument7 pagesIelts Task 2 6 Sample EssaysSungjin ParkNo ratings yet
- As Children Become AdultsDocument1 pageAs Children Become AdultsHadil AltilbaniNo ratings yet
- Sodium Hypochlorite inDocument13 pagesSodium Hypochlorite inDr.O.R.GANESAMURTHINo ratings yet
- Aetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailDocument10 pagesAetiology of Root Canal Treatment Failure - Why Well-Treated Teeth Can FailFlorin IonescuNo ratings yet
- JofIMAB - 2014 20 1p490 493Document4 pagesJofIMAB - 2014 20 1p490 493Hadil AltilbaniNo ratings yet
- Radiographic monitoring vs retreatment for deficient root fillingsDocument8 pagesRadiographic monitoring vs retreatment for deficient root fillingsRest0No ratings yet
- Morita Endo Comp enDocument10 pagesMorita Endo Comp enHadil AltilbaniNo ratings yet
- RSBO v8n3 Artigo12Document8 pagesRSBO v8n3 Artigo12Hadil AltilbaniNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- EndoDocument61 pagesEndodeenm100% (2)
- Diabetes MellitusDocument9 pagesDiabetes MellitusHadil AltilbaniNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Guidelines for Surgical Endodontic ProceduresDocument11 pagesGuidelines for Surgical Endodontic ProceduresgrzeniouNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- CrownDocument27 pagesCrownHadil Altilbani100% (1)
- Protozoa: Single-Celled Microscopic OrganismsDocument21 pagesProtozoa: Single-Celled Microscopic Organismsrimisha raimaNo ratings yet
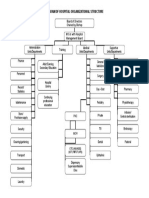
- Diagram of Hospital Organizational Structure: Board of Directors Chaired by Bishop MO I/c With Hospital Management BoardDocument1 pageDiagram of Hospital Organizational Structure: Board of Directors Chaired by Bishop MO I/c With Hospital Management BoardBELAY AWOKENo ratings yet
- chapter-4-ACELLULAR AND PROKARYOTIK MICROBESDocument66 pageschapter-4-ACELLULAR AND PROKARYOTIK MICROBESCza Mae ArsenalNo ratings yet
- Peds Clipp Cases NotesDocument5 pagesPeds Clipp Cases NotesLauren LevyNo ratings yet
- CDN Post Test Answer KeyDocument5 pagesCDN Post Test Answer KeyCharme Jean Raygon100% (1)
- Aseptic TechniqueDocument571 pagesAseptic TechniqueNadhiya Ealumalai0% (1)
- Lonza BenchGuides Poietics Human Immune System CellsDocument1 pageLonza BenchGuides Poietics Human Immune System CellsManoj Kumar pandreNo ratings yet
- Grammar and Spelling QuizDocument10 pagesGrammar and Spelling QuizKamsani MuhammadNo ratings yet
- COVID-19 Pandemic: Coronavirus Pandemic, Is An Ongoing GlobalDocument86 pagesCOVID-19 Pandemic: Coronavirus Pandemic, Is An Ongoing GlobalXx XxNo ratings yet
- COVID-19 Pandemic in India: Present Scenario and A Steep Climb AheadDocument4 pagesCOVID-19 Pandemic in India: Present Scenario and A Steep Climb AheadSafikul HossainNo ratings yet
- Doctor Who Identified SARS Becomes Its Victim - Elementary PDFDocument5 pagesDoctor Who Identified SARS Becomes Its Victim - Elementary PDFhahahapsu100% (1)
- Katzung CaculsDocument156 pagesKatzung CaculsBrionelle DumelodNo ratings yet
- Pertemuan 15 - Epidemiologi Penyakit New Emerging DiseaseDocument79 pagesPertemuan 15 - Epidemiologi Penyakit New Emerging DiseasePutti AnnisaNo ratings yet
- Texas West Nile Outbreak Most Deadly in The NationDocument11 pagesTexas West Nile Outbreak Most Deadly in The NationmfadegreeNo ratings yet
- A Brief Note On: Chicken PoxDocument29 pagesA Brief Note On: Chicken PoxRemesh ChandranNo ratings yet
- Signs and Symptoms of AppendicitisDocument17 pagesSigns and Symptoms of AppendicitisMarge Orge100% (1)
- Nail Care Tools and EquipmentDocument36 pagesNail Care Tools and EquipmentArnoldtin TheanadineNo ratings yet
- Introduction To VirologyDocument22 pagesIntroduction To VirologymicroperadeniyaNo ratings yet
- Typhoid FeverDocument4 pagesTyphoid FeverBernice GyapongNo ratings yet
- Epidemiologi of HFMDDocument16 pagesEpidemiologi of HFMDJimmy AmbaritaNo ratings yet
- Mda Palakkad 2016 NewDocument33 pagesMda Palakkad 2016 NewAasifKNazarNo ratings yet
- 1 The History and Scope of Microbiology Rev3 090216Document45 pages1 The History and Scope of Microbiology Rev3 090216HairunnisaNo ratings yet
- New Microsoft Word DocumentDocument19 pagesNew Microsoft Word DocumentAisha FakhryNo ratings yet
- Microbiology 2013Document7 pagesMicrobiology 2013kriss Wong50% (2)
- Immun e System: Chapter 31.2 Page 885Document21 pagesImmun e System: Chapter 31.2 Page 885JanaNo ratings yet
- Micropara ReviewerDocument12 pagesMicropara ReviewerAlyssa Mae Azarcon100% (1)
- هيئهDocument24 pagesهيئهNane050No ratings yet
- The Corrupted Blood IncidentDocument13 pagesThe Corrupted Blood IncidentGabriel Andrei StanNo ratings yet
- Nursing Care PlanDocument10 pagesNursing Care PlanElijah S GomezNo ratings yet
- Role of Chitin in Fungal Pathogenesis and Immune ResponseDocument66 pagesRole of Chitin in Fungal Pathogenesis and Immune Responseharisath2003100% (1)