You might also like
- General Conditions of Contract For Construction Works 3rd Edition 2015Document139 pagesGeneral Conditions of Contract For Construction Works 3rd Edition 2015Kathryn Verhagen100% (11)
- The Oprah Magazine 2010-01Document167 pagesThe Oprah Magazine 2010-01juscoNo ratings yet
- Chapter 3 GEDocument15 pagesChapter 3 GEashasyraaf0% (1)
- Law ReportDocument41 pagesLaw ReportJoshua ChongNo ratings yet
- OHS Body of Knowledge Risk April, 2012Document50 pagesOHS Body of Knowledge Risk April, 2012Nadia Nur GhaniaNo ratings yet
- 26 Hazard Thermal Environment PDFDocument39 pages26 Hazard Thermal Environment PDFamirq4No ratings yet
- Synopsis: Core Body of Knowledge For The Generalist OHS ProfessionalDocument5 pagesSynopsis: Core Body of Knowledge For The Generalist OHS Professionalinneke mutiaraNo ratings yet
- 16 Hazard Biomechanical PDFDocument26 pages16 Hazard Biomechanical PDFamirq4No ratings yet
- 30 Hazard Vehicles and Occupational Road Use PDFDocument31 pages30 Hazard Vehicles and Occupational Road Use PDFamirq4No ratings yet
- 24 Hazard Ionising Radiation PDFDocument32 pages24 Hazard Ionising Radiation PDFamirq4No ratings yet
- 9 Sociopolitical Industrial PDFDocument28 pages9 Sociopolitical Industrial PDFamirq4No ratings yet
- 22 Hazard Noise PDFDocument40 pages22 Hazard Noise PDFamirq4No ratings yet
- 3 The Generalist OHS ProfessionalDocument52 pages3 The Generalist OHS Professionalamirq4No ratings yet
- 20 FatigueDocument28 pages20 FatigueAndres Lucero LeivaNo ratings yet
- 35 Control Mitigation Emergency PreparednessDocument25 pages35 Control Mitigation Emergency PreparednessTri SubaktiNo ratings yet
- Occupational Health and Safety SystemsDocument31 pagesOccupational Health and Safety Systemsbeershebak2707No ratings yet
- 28 Hazard Plant PDFDocument28 pages28 Hazard Plant PDFJohn Paul GonzalesNo ratings yet
- 37 Introduction To Practice As A ConceptDocument10 pages37 Introduction To Practice As A ConceptDea Yasmine ArmandoNo ratings yet
- 6 Global Health PDFDocument25 pages6 Global Health PDFNobella Arifannisa FirdausiNo ratings yet
- 8.2 Principles of OHS Law FinalDocument35 pages8.2 Principles of OHS Law FinalJackson Musonda KapilyaNo ratings yet
- Achieving Excellence Guide Risk & Value ManagementDocument24 pagesAchieving Excellence Guide Risk & Value ManagementsizwehNo ratings yet
- Assessment of Human Factors On Oil SpillsDocument53 pagesAssessment of Human Factors On Oil SpillsflouzanNo ratings yet
- Behaviour-Based Safety in Organizations: Saving Life Before The Accident, 2/eDocument2 pagesBehaviour-Based Safety in Organizations: Saving Life Before The Accident, 2/ePampanagouda YadavNo ratings yet
- IOSHCPD Export 2021-09-07 03 58 43Document1 pageIOSHCPD Export 2021-09-07 03 58 43besongNo ratings yet
- Difference Between ClausesDocument4 pagesDifference Between ClausesNash C. UsopNo ratings yet
- Ehandbook Process Safety 1309 PDFDocument15 pagesEhandbook Process Safety 1309 PDFArun KumarNo ratings yet
- Safety Culture AssesmentDocument2 pagesSafety Culture AssesmentfaradayzzzNo ratings yet
- Popular Leadership StylesDocument2 pagesPopular Leadership StylesLalit JhaNo ratings yet
- SafetyRiskManagementProcess Anglo American TheKeytoZeroHarmDocument38 pagesSafetyRiskManagementProcess Anglo American TheKeytoZeroHarmEdgardo Ismael Ramos PumacahuaNo ratings yet
- Events and Causal Factors Analysis: DescriptionDocument3 pagesEvents and Causal Factors Analysis: DescriptionChristopher YsitNo ratings yet
- Standart Anzi Eyewash PDFDocument12 pagesStandart Anzi Eyewash PDFDwiki Yanuar Ramadhan100% (1)
- Behavioural Safety and CultureDocument45 pagesBehavioural Safety and CulturergadeamerinoNo ratings yet
- Risk Assessment 2-SupplementDocument42 pagesRisk Assessment 2-SupplementadityaNo ratings yet
- Safety Science: David Oswald, Fred Sherratt, Simon SmithDocument11 pagesSafety Science: David Oswald, Fred Sherratt, Simon SmithFatih D. PrasetioNo ratings yet
- Safety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 2 Safety CultureDocument32 pagesSafety Behaviours: Human Factors For Pilots 2nd Edition: Resource Booklet 2 Safety CultureSonya McSharkNo ratings yet
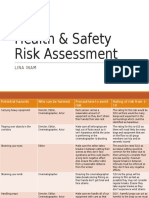
- Health & Safety Risk AssessmentDocument2 pagesHealth & Safety Risk AssessmentLina Inam100% (1)
- Safety Culture A Framework For ImprovementDocument85 pagesSafety Culture A Framework For Improvementrmallorca777100% (1)
- Facilitator's Guide: Behavioural SafetyDocument21 pagesFacilitator's Guide: Behavioural Safetyvbnaik03No ratings yet
- 3.modul Safety LeadershipDocument43 pages3.modul Safety LeadershipmusaNo ratings yet
- Guide For The Evaluation of Fire Risk Assessments 2016 EditionDocument23 pagesGuide For The Evaluation of Fire Risk Assessments 2016 EditionSimone DoeNo ratings yet
- N 06300 IP1038 Human Factors Competancy Assurance Rev 0 Dec 2012 PDFDocument12 pagesN 06300 IP1038 Human Factors Competancy Assurance Rev 0 Dec 2012 PDFsubragkNo ratings yet
- Safety Leadership NewDocument35 pagesSafety Leadership NewdhabriNo ratings yet
- Human Factors in The Management of Major Accident HazardsDocument8 pagesHuman Factors in The Management of Major Accident HazardsAnonymous FmXEu2cHxKNo ratings yet
- Qualitative V Quantitative Risk AssessmentDocument5 pagesQualitative V Quantitative Risk AssessmentGundeepNo ratings yet
- 02 02 OrganizingDocument27 pages02 02 OrganizingrpjongNo ratings yet
- Key Note Safety LeadershipDocument33 pagesKey Note Safety LeadershipRiko Adi SunaryoNo ratings yet
- 501 2012 6 28 27 39 561Document26 pages501 2012 6 28 27 39 561MITHILESH KUMARNo ratings yet
- Behavior-Based Safety: All in The FamilyDocument2 pagesBehavior-Based Safety: All in The FamilyPipat Singha-inNo ratings yet
- Ramp Safety CultureDocument11 pagesRamp Safety CultureRumesh ThilakarathnaNo ratings yet
- 2017 Safety Awards Descriptions ApplicationDocument3 pages2017 Safety Awards Descriptions ApplicationFahryan RozakNo ratings yet
- A Method For Root Cause Analysis With A Bayesian Belief Network and Fuzzy Cognitive Map PDFDocument20 pagesA Method For Root Cause Analysis With A Bayesian Belief Network and Fuzzy Cognitive Map PDFAndrea CalderaNo ratings yet
- INSHPO 2017 Capability Framework Final PDFDocument48 pagesINSHPO 2017 Capability Framework Final PDFTamikNo ratings yet
- Idse Unit 2Document207 pagesIdse Unit 2farhan AliNo ratings yet
- BowTie Risk AssessmentDocument21 pagesBowTie Risk AssessmentSofia Maan Guinto100% (1)
- The Management of Occupational Health and Safety in The South African Mining Industry 04 12 2018Document34 pagesThe Management of Occupational Health and Safety in The South African Mining Industry 04 12 2018LeeLowersNo ratings yet
- Leadership Principles For Building An Ideal Safety Culture: Complimentary Webinar: 12/7/2021Document75 pagesLeadership Principles For Building An Ideal Safety Culture: Complimentary Webinar: 12/7/2021mjbotelhoNo ratings yet
- Sample IA GUIDEDocument7 pagesSample IA GUIDEAmalNo ratings yet
- Practical Guide To Safety Leadership - An Evidence Based ApproachDocument205 pagesPractical Guide To Safety Leadership - An Evidence Based Approachtyo100% (2)
- What Are The Characteristics of High Reliability Organizations? - The 5 Pillars of The U.S. Navy's Nuclear Propulsion ProgramDocument1 pageWhat Are The Characteristics of High Reliability Organizations? - The 5 Pillars of The U.S. Navy's Nuclear Propulsion ProgramWilson Perumal & CompanyNo ratings yet
- 34 Control Prevention and InterventionDocument35 pages34 Control Prevention and InterventionAmi NuariNo ratings yet
- 29 Hazard Mobile Plant PDFDocument25 pages29 Hazard Mobile Plant PDFamirq4100% (1)
- 28 Hazard Plant PDFDocument28 pages28 Hazard Plant PDFamirq4No ratings yet
- Sesi 6 12.1 SystemsDocument31 pagesSesi 6 12.1 SystemsWafiq Febri Erlianti SafitriNo ratings yet
- 21 Hazard Bullying PDFDocument45 pages21 Hazard Bullying PDFamirq4No ratings yet
- InterpretingDocument41 pagesInterpretingprenatooliveiraNo ratings yet
- D 6584 - 00 - Rdy1odqDocument5 pagesD 6584 - 00 - Rdy1odqSeven DangNo ratings yet
- EN ISO 11357-1: Plastics - Differential Scanning Calorimetry (DSC)Document14 pagesEN ISO 11357-1: Plastics - Differential Scanning Calorimetry (DSC)juscoNo ratings yet
- Fewer Gels MeanDocument2 pagesFewer Gels MeanjuscoNo ratings yet
- Cinnamon and Cream Cheese MacaronsDocument1 pageCinnamon and Cream Cheese MacaronsjuscoNo ratings yet
- Wo He Dec 2010Document156 pagesWo He Dec 2010juscoNo ratings yet
- Dramatica Theory BookDocument343 pagesDramatica Theory BookIván Falcón100% (1)
- Rajiv Thapar v. Madan Lal Kapoor PDFDocument23 pagesRajiv Thapar v. Madan Lal Kapoor PDFgunjeet singhNo ratings yet
- Financial Reporting and Analysis Revsine 6th Edition Solutions ManualDocument16 pagesFinancial Reporting and Analysis Revsine 6th Edition Solutions Manualweantoss8ykg5100% (42)
- (Download PDF) Between Debt and The Devil Money Credit and Fixing Global Finance Turner Online Ebook All Chapter PDFDocument40 pages(Download PDF) Between Debt and The Devil Money Credit and Fixing Global Finance Turner Online Ebook All Chapter PDFjasmine.newburn311No ratings yet
- Psychology An Introduction 10th Edition Lahey Test BankDocument26 pagesPsychology An Introduction 10th Edition Lahey Test Bankdictumhuronianhsor100% (18)
- Complete Consent Form UW School of DentistryDocument13 pagesComplete Consent Form UW School of DentistryBryaniNo ratings yet
- Reading & Writing WK 2Document8 pagesReading & Writing WK 2JeninaS.Lim100% (2)
- Copyright Infringement Lawsuit COMPLAINT DISTURBIA Movie Against Steven Spielberg UniversalDocument60 pagesCopyright Infringement Lawsuit COMPLAINT DISTURBIA Movie Against Steven Spielberg UniversalpacketfireNo ratings yet
- Audi A5 2016 CameraDocument8 pagesAudi A5 2016 CameraTung NguyenNo ratings yet
- GROUP 2014 Users ManualDocument676 pagesGROUP 2014 Users ManualLea MarselaNo ratings yet
- RM Mod5Document20 pagesRM Mod5bhoomibhaskar23No ratings yet
- White v. West (SDNY)Document14 pagesWhite v. West (SDNY)sstithamNo ratings yet
- Protection of Traditional Cultural Expressions by IP RightsDocument13 pagesProtection of Traditional Cultural Expressions by IP RightsAlex John HarrisonNo ratings yet
- Cutter, Benjamin - How To Study Kreutzer PDFDocument71 pagesCutter, Benjamin - How To Study Kreutzer PDFvivaldiozNo ratings yet
- Tutorial Programa AGEDocument34 pagesTutorial Programa AGEDanilo VegaNo ratings yet
- A Vanished Arcadia: Being Some Account of The Jesuits in Paraguay 1607-1767 by Cunninghame Graham, R. B. (Robert Bontine), 1852-1936Document159 pagesA Vanished Arcadia: Being Some Account of The Jesuits in Paraguay 1607-1767 by Cunninghame Graham, R. B. (Robert Bontine), 1852-1936Gutenberg.orgNo ratings yet
- An Ideal KitchenDocument29 pagesAn Ideal KitchenBillNo ratings yet
- Read Online Textbook Pill Hill Bryan W Dull Ebook All Chapter PDFDocument20 pagesRead Online Textbook Pill Hill Bryan W Dull Ebook All Chapter PDFjose.thomas601100% (3)
- Ll.m. Syllabus - Intellectual Property LawDocument60 pagesLl.m. Syllabus - Intellectual Property Lawananthineevs7btsNo ratings yet
- 6881005y52 o PDFDocument157 pages6881005y52 o PDFMike MeronNo ratings yet
- R AgreementDocument4 pagesR AgreementMasum SharifNo ratings yet
- The Primitive Church and The SeeDocument537 pagesThe Primitive Church and The Seemongladz3468No ratings yet
- Hiertest RAK Lab 16.1Document41 pagesHiertest RAK Lab 16.1Veeranjaneyulu Dhikonda100% (1)
- FX Inside FIX Client API 3.9.5v1Document154 pagesFX Inside FIX Client API 3.9.5v1ps4scribdNo ratings yet
- CombinepdfDocument120 pagesCombinepdfFurious GraveNo ratings yet
- PT030000 Relatedresources 2016CopyrightDevelopmentsDocument762 pagesPT030000 Relatedresources 2016CopyrightDevelopmentsJohnNo ratings yet