You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Formula Writing - CambridgeDocument5 pagesFormula Writing - CambridgeQusai Saify100% (3)
- Procedure Natural Gas Piping Purging HazardsDocument4 pagesProcedure Natural Gas Piping Purging HazardsEko KurniawanNo ratings yet
- 03 Blending PowerpointDocument70 pages03 Blending PowerpointNinhHoàngHải100% (4)
- Chemistry Investigatory ProjectDocument19 pagesChemistry Investigatory ProjectDivya Vatsa50% (4)
- Solar Stills For Desalination of Water in Rural Households: Amitava BhattacharyyaDocument10 pagesSolar Stills For Desalination of Water in Rural Households: Amitava BhattacharyyaTrimo Wahyu Bimantoro100% (1)
- Models For Volcanic-Hosted Epithermal Precious Metal Deposits A ReviewDocument11 pagesModels For Volcanic-Hosted Epithermal Precious Metal Deposits A ReviewOrlando B Santa CruzNo ratings yet
- Color, Solubility, and Complex Ion Equilibria of Nickel (11) Species in Aqueous SolutionDocument2 pagesColor, Solubility, and Complex Ion Equilibria of Nickel (11) Species in Aqueous SolutionManuel OrihuelaNo ratings yet
- SRMB SteelDocument31 pagesSRMB SteelAmol Ujawane100% (1)
- Ques Paper 2-XI-ENGDocument8 pagesQues Paper 2-XI-ENGKrish VermaNo ratings yet
- 202 Introduction To Materials ScienceDocument435 pages202 Introduction To Materials ScienceRK SinghNo ratings yet
- Sample Problem 1: X Direction X Direction XDocument4 pagesSample Problem 1: X Direction X Direction XHarold MangaNo ratings yet
- BLASTING &PRIMER ProtocolDocument104 pagesBLASTING &PRIMER ProtocolSulekh GhoshNo ratings yet
- BelgJBotJansenetal1998 PDFDocument10 pagesBelgJBotJansenetal1998 PDFalexNo ratings yet
- Spectracron 110 FD Alkyd Enamel PDFDocument2 pagesSpectracron 110 FD Alkyd Enamel PDFSatish Vishnubhotla0% (1)
- Advances in Vapor Compression Technology For The Production of USP Purified Water and Water For InjectionDocument8 pagesAdvances in Vapor Compression Technology For The Production of USP Purified Water and Water For InjectionTimNo ratings yet
- ManometerDocument2 pagesManometerAlexanderSorianoNo ratings yet
- Glass Ceramics QuizDocument3 pagesGlass Ceramics QuizRon Pascual100% (1)
- Elvaloy 4170 Research PaperDocument4 pagesElvaloy 4170 Research PaperGolam MasudNo ratings yet
- S Start of Lesson E End of Lesson Grading 1-5: Learning Outcomes Progress ArrowDocument30 pagesS Start of Lesson E End of Lesson Grading 1-5: Learning Outcomes Progress ArrowYu Seung KimNo ratings yet
- NDT-SA-ARAMCO-MCCL-PT-57 Rev 00-Date-26-June-2023Document20 pagesNDT-SA-ARAMCO-MCCL-PT-57 Rev 00-Date-26-June-2023SANJEEV YADAVNo ratings yet
- PNS BAFS 183 2020 Organic Soil AmendmentsDocument14 pagesPNS BAFS 183 2020 Organic Soil Amendmentsjeffrey sarolNo ratings yet
- 2002Document38 pages2002B GirishNo ratings yet
- Topic 4: Classification, Properties and Applications of S.G. and C.G.Iron S.G.IRONDocument11 pagesTopic 4: Classification, Properties and Applications of S.G. and C.G.Iron S.G.IRONsandeep kumarNo ratings yet
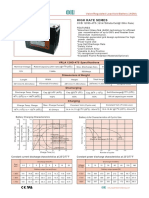
- High Rate Series: CCB 12HD-475Document1 pageHigh Rate Series: CCB 12HD-475orunmila123No ratings yet
- Shell Gadus S2 OG Clear Oil 20000Document2 pagesShell Gadus S2 OG Clear Oil 20000Xavier DiazNo ratings yet
- A Case Study On Solar Vapour Absorption Refrigeration SystemDocument7 pagesA Case Study On Solar Vapour Absorption Refrigeration SystemShivam MaheraNo ratings yet
- Extintor CO2 B10V-1 - BADGER PDFDocument2 pagesExtintor CO2 B10V-1 - BADGER PDFCoordinador TecnicoNo ratings yet
- ACS Sustainable Chemistry & Engineering - 2020Document9 pagesACS Sustainable Chemistry & Engineering - 2020Eugene YiNo ratings yet
- Jotafloor TC EDocument6 pagesJotafloor TC ERidwanSalminNo ratings yet
- Cod and BodDocument57 pagesCod and Boddinesh kumarNo ratings yet