You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- PHYSIOLOGY OF PREGNANCYDocument50 pagesPHYSIOLOGY OF PREGNANCYEvy Wulandari100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PICU HandbookDocument113 pagesPICU HandbookEdu WilliamNo ratings yet
- Mahmood Shafi, Helen Bolton, Ketankumar Gajjar (Eds.) - Gynaecological Oncology For The MRCOG-Cambridge University Press (2018) PDFDocument226 pagesMahmood Shafi, Helen Bolton, Ketankumar Gajjar (Eds.) - Gynaecological Oncology For The MRCOG-Cambridge University Press (2018) PDFprimadian atnaryanNo ratings yet
- Nurse's Pocket GuideDocument11 pagesNurse's Pocket GuideRaf_Harold_427No ratings yet
- Exp 3Document7 pagesExp 3Chan Wei QuanNo ratings yet
- CroupDocument13 pagesCroupEdu William100% (1)
- PediatricsDocument79 pagesPediatricsapi-3712326No ratings yet
- Psychogenic VomitingDocument3 pagesPsychogenic VomitingMylene Jane Husain Bartolome100% (1)
- Pedtext 5Document716 pagesPedtext 5jay_eshwa100% (1)
- Play in Child Development andDocument194 pagesPlay in Child Development andAlinaZbarloiu100% (4)
- Is There A Role For Transversus Abdominis in Lumbo-Pelvic Stability?Document13 pagesIs There A Role For Transversus Abdominis in Lumbo-Pelvic Stability?mientwegNo ratings yet
- @medicalbookpdf Preeclampsia PDFDocument286 pages@medicalbookpdf Preeclampsia PDFgalihsupanji111_2230No ratings yet
- Delivery Room RequirementsDocument12 pagesDelivery Room RequirementsHannah Ros Quitorio IINo ratings yet
- 2 Salivary GlandsDocument20 pages2 Salivary GlandsKaty SanchezNo ratings yet
- Guidelines For CHPS ImplementationDocument16 pagesGuidelines For CHPS ImplementationErasmus Agongo100% (1)
- OCB Cataract Surgery QA BookletDocument36 pagesOCB Cataract Surgery QA BookletSurendar KesavanNo ratings yet
- Wound International Best Practice Guidelines Non ComplexDocument27 pagesWound International Best Practice Guidelines Non ComplexEdu WilliamNo ratings yet
- 2000 Trauma ManagementDocument691 pages2000 Trauma ManagementSon Nguyen100% (4)
- Kjeldsberg Chap 1Document14 pagesKjeldsberg Chap 1Joyee BasuNo ratings yet
- Adolescent Medicine IDocument45 pagesAdolescent Medicine Iapi-3712326100% (1)
- Dietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Document1 pageDietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Edu WilliamNo ratings yet
- PALS Manual Changes January 2012Document1 pagePALS Manual Changes January 2012Danhil RamosNo ratings yet
- Laser Guidance Notes 101212Document3 pagesLaser Guidance Notes 101212Edu WilliamNo ratings yet
- Fast Food For Our Preemies .3Document2 pagesFast Food For Our Preemies .3Edu WilliamNo ratings yet
- Modified Finnegan ScoringDocument4 pagesModified Finnegan ScoringEdu WilliamNo ratings yet
- Membaca EkgDocument90 pagesMembaca EkgEdu WilliamNo ratings yet
- Pressure Ulcer Assessment CardDocument2 pagesPressure Ulcer Assessment CardEdu WilliamNo ratings yet
- General PediatricsDocument36 pagesGeneral PediatricsEdu WilliamNo ratings yet
- Tanner MethodDocument8 pagesTanner MethodEdu WilliamNo ratings yet
- 12 - Asthma PDFDocument21 pages12 - Asthma PDFjuniorebindaNo ratings yet
- Amnioinfusion For The Prevention of MASDocument9 pagesAmnioinfusion For The Prevention of MASEdu WilliamNo ratings yet
- Body Size in DHFDocument6 pagesBody Size in DHFEdu WilliamNo ratings yet
- Asthma v.3.0: Criteria and Respiratory ScoreDocument36 pagesAsthma v.3.0: Criteria and Respiratory ScoreYudha Astipamara PanjayaNo ratings yet
- Field Guide to Surveillance of Acute Flaccid ParalysisDocument49 pagesField Guide to Surveillance of Acute Flaccid ParalysissmopunhnanaNo ratings yet
- Pediatric Surgery HandbookDocument29 pagesPediatric Surgery HandbookEdu WilliamNo ratings yet
- MMRVDocument2 pagesMMRVMichael HalimNo ratings yet
- Pert PDFDocument18 pagesPert PDFKhalilah AisyahNo ratings yet
- HPV (Gardasil) - 2011Document2 pagesHPV (Gardasil) - 2011Edu WilliamNo ratings yet
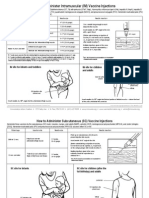
- How to Administer IM and SC Vaccine InjectionsDocument2 pagesHow to Administer IM and SC Vaccine InjectionsEdu WilliamNo ratings yet
- Japanese Encephalitis - 2011Document2 pagesJapanese Encephalitis - 2011Edu WilliamNo ratings yet
- State of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthDocument228 pagesState of The World's Midwifery 2014: A Universal Pathway - A Woman's Right To HealthUNFPA SoWMYNo ratings yet
- Drug Study: Cavite State University (Cvsu)Document2 pagesDrug Study: Cavite State University (Cvsu)Angelica Cassandra VillenaNo ratings yet
- Ethical and Legal Issues in Reproductive HealthDocument4 pagesEthical and Legal Issues in Reproductive HealthBianca_P0pNo ratings yet
- Anna Eakes - Reflection PaperDocument7 pagesAnna Eakes - Reflection Paperapi-558091839No ratings yet
- Borang Permohonan Pegawai Perubatan Lantikan Secara Multiple Entry (Warganegara) Di Kementerian Kesihatan MalaysiaDocument15 pagesBorang Permohonan Pegawai Perubatan Lantikan Secara Multiple Entry (Warganegara) Di Kementerian Kesihatan MalaysiaHafiz IbrahimNo ratings yet
- Challenges in Implementing Innovations in Midwifery Practice An OverviewDocument3 pagesChallenges in Implementing Innovations in Midwifery Practice An OverviewEditor IJTSRDNo ratings yet
- Emergency Drug ListDocument17 pagesEmergency Drug ListLala Rahma Qodriyan SofiakmiNo ratings yet
- Shoulder Presentation Diagnosis and ManagementDocument20 pagesShoulder Presentation Diagnosis and ManagementCrevins NyarikiNo ratings yet
- Rotary Club of Kampala Naalya BulletinDocument4 pagesRotary Club of Kampala Naalya BulletinDenis JjuukoNo ratings yet
- Meconium Aspiration SyndromeDocument7 pagesMeconium Aspiration SyndromeAi Niech Inoel100% (1)
- Dopamine release stimulant and Ligase inhibitor effects and targetsDocument59 pagesDopamine release stimulant and Ligase inhibitor effects and targetsapoorva_1989No ratings yet
- Treating Deep Overbite MalocclusionDocument1 pageTreating Deep Overbite MalocclusionZhyema ZhyedeeNo ratings yet
- MTurbo System SpecificationDocument2 pagesMTurbo System SpecificationSerban MihaelaNo ratings yet
- Al Manar Hospital Mohammadpur Doctor List & ContactDocument1 pageAl Manar Hospital Mohammadpur Doctor List & Contactrubayat112015No ratings yet
- Definisi Dan Kriteria Terbaru Diagnosis Sepsis Sepsis-3Document5 pagesDefinisi Dan Kriteria Terbaru Diagnosis Sepsis Sepsis-3nindyaNo ratings yet
- Lower Extremity Venous Duplex USDocument6 pagesLower Extremity Venous Duplex USjmg_mdNo ratings yet
- Australian Spelling ListDocument35 pagesAustralian Spelling ListKiruba JacobNo ratings yet
- Initiating, Maintaining and Terminating Blood Transfusion ProceduresDocument1 pageInitiating, Maintaining and Terminating Blood Transfusion ProceduresCarol Neng CalupitanNo ratings yet
- BreechDocument50 pagesBreechEldrinAbquinaNo ratings yet