You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ben'S Muffler RepairDocument9 pagesBen'S Muffler RepairDana LantoNo ratings yet
- Brooks MT 3018Document16 pagesBrooks MT 3018Martin AndradeNo ratings yet
- CBT Perspectives Aug 2015 EditorialDocument3 pagesCBT Perspectives Aug 2015 EditorialHadi M. KuriryNo ratings yet
- Residents' Duty Hours - Toward An Empirical NarrativeDocument6 pagesResidents' Duty Hours - Toward An Empirical NarrativeHadi M. KuriryNo ratings yet
- Mucosa-Associated Lymphoid Tissue Lymphoma Presenting As Massive Gastrointestinal Bleeding: A Case ReportDocument5 pagesMucosa-Associated Lymphoid Tissue Lymphoma Presenting As Massive Gastrointestinal Bleeding: A Case ReportHadi M. KuriryNo ratings yet
- Ann Oncol 2012 ضberg Vii124 30Document7 pagesAnn Oncol 2012 ضberg Vii124 30Hadi M. KuriryNo ratings yet
- Gastroenterol. Rep. 2014 Zacharia 154 7Document4 pagesGastroenterol. Rep. 2014 Zacharia 154 7Hadi M. KuriryNo ratings yet
- 05 Rajasekhar DiscardIIDocument5 pages05 Rajasekhar DiscardIIHadi M. KuriryNo ratings yet
- Introduction NETDocument3 pagesIntroduction NETHadi M. KuriryNo ratings yet
- GH 05 839Document12 pagesGH 05 839Hadi M. KuriryNo ratings yet
- DettolDocument3 pagesDettolShantanuNo ratings yet
- 2011 Article 1952Document7 pages2011 Article 1952Hadi M. KuriryNo ratings yet
- Primary Gastrointestinal Lymphoma in Japan 2003Document12 pagesPrimary Gastrointestinal Lymphoma in Japan 2003Nora RamkitaNo ratings yet
- 10 1 1 356 6862Document4 pages10 1 1 356 6862Hadi M. KuriryNo ratings yet
- CopdDocument10 pagesCopdHadi M. KuriryNo ratings yet
- Hepatocellular Carcinoma in The United States. Lessons From A Population-Based Study in Medicare RecipientsDocument3 pagesHepatocellular Carcinoma in The United States. Lessons From A Population-Based Study in Medicare RecipientsHadi M. KuriryNo ratings yet
- 1 s2.0 S0168827805006616 MainDocument9 pages1 s2.0 S0168827805006616 MainHadi M. KuriryNo ratings yet
- Diag MNG Neuro TumorsDocument10 pagesDiag MNG Neuro TumorsHadi M. KuriryNo ratings yet
- Diag MNG Neuro TumorsDocument10 pagesDiag MNG Neuro TumorsHadi M. KuriryNo ratings yet
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- Ecl7000 enDocument2 pagesEcl7000 ensuchaya tupyangNo ratings yet
- Plano Grupo ElectrogenoDocument2 pagesPlano Grupo Electrogenoluis alberto rodriguezNo ratings yet
- Basic Science JSS 1 2NDDocument29 pagesBasic Science JSS 1 2NDAdeoye Olufunke100% (2)
- Dapsone 2Document2 pagesDapsone 2JeanMENo ratings yet
- School and CentreDocument24 pagesSchool and CentreThrilling PrinceNo ratings yet
- Worlds Healthiest Super Food - SpirulinaDocument16 pagesWorlds Healthiest Super Food - SpirulinaBhadra BasumataryNo ratings yet
- Codex CRD26Document9 pagesCodex CRD26arely svetlana gaspar badilloNo ratings yet
- Planet X Restaurant Menu v2Document5 pagesPlanet X Restaurant Menu v2Chinthaka WilliamsNo ratings yet
- ARTIKEL 44 Famuntamah 391-399Document9 pagesARTIKEL 44 Famuntamah 391-399Dandi Aksan MasjudNo ratings yet
- Handling Silica in Cooling WaterDocument17 pagesHandling Silica in Cooling WaterLekhamani YadavNo ratings yet
- Health Behaviour: Current Issues and ChallengesDocument13 pagesHealth Behaviour: Current Issues and ChallengesK.A.No ratings yet
- CHEMDocument20 pagesCHEMValli RamalingamNo ratings yet
- Oil Record Book InstructionsDocument6 pagesOil Record Book InstructionsNamal Fernando100% (1)
- MEH B1 Video Book Answer KeyDocument6 pagesMEH B1 Video Book Answer KeyTru CallingNo ratings yet
- TS68Document52 pagesTS68finandariefNo ratings yet
- Individual Differences and Personality in "Ugly Betty", S01E01Document6 pagesIndividual Differences and Personality in "Ugly Betty", S01E01Starling HunterNo ratings yet
- RR No. 6-2015 PDFDocument5 pagesRR No. 6-2015 PDFErlene CompraNo ratings yet
- Project: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectDocument26 pagesProject: M/S Cae-Gondia at Nagpur Cable Schedule For Proposed ProjectMurali MohanNo ratings yet
- The Suitcase ProjectDocument27 pagesThe Suitcase Projectshubhamkumar9211No ratings yet
- Broiled Salisbury SteaksDocument29 pagesBroiled Salisbury SteaksCei mendozaNo ratings yet
- Heat Transfer Surfaces Guide PDFDocument8 pagesHeat Transfer Surfaces Guide PDFJohan ConradieNo ratings yet
- Warm Vs Cold ShockDocument8 pagesWarm Vs Cold ShockmarleeramirezNo ratings yet
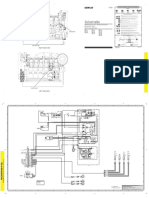
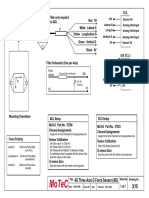
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet
- Concrete Pump Hose TDSDocument2 pagesConcrete Pump Hose TDSAlaa Abu KhurjNo ratings yet
- Curriculum DesignDocument20 pagesCurriculum DesignRose Glaire Alaine TabraNo ratings yet
- NSEA Solved Paper 2015Document30 pagesNSEA Solved Paper 2015vv12345670% (1)
- Shall We Date Obey Me! - Works Archive of Our OwnDocument1 pageShall We Date Obey Me! - Works Archive of Our OwnEdyn LaiNo ratings yet
- Manual Book IOG ConventionDocument17 pagesManual Book IOG ConventionTaufiq MaulanaNo ratings yet