You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fitzpatrick Skin Type Classification ScaleDocument3 pagesFitzpatrick Skin Type Classification ScaleHanarisha Putri AzkiaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The JCI Big Book of ChecklistDocument150 pagesThe JCI Big Book of ChecklistMiguel Angel Chávez88% (8)
- EcgDocument18 pagesEcgDelyn Gamutan MillanNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Performance Improvement Plan Template 1 - 908445459Document3 pagesPerformance Improvement Plan Template 1 - 908445459api-534828007No ratings yet
- Single Tooth ImplantsDocument95 pagesSingle Tooth ImplantsRavinder NarwalNo ratings yet
- RCGP NSPCC Safeguarding Children ToolkitDocument223 pagesRCGP NSPCC Safeguarding Children ToolkitMirela Cojocaru StetcoNo ratings yet
- Perforative PeritonitisDocument58 pagesPerforative PeritonitisSangeeta BSR82% (17)
- Imci Case StudyDocument10 pagesImci Case StudyRhika Mae Flores Valdez100% (1)
- The Mechanism of Wound HealingDocument17 pagesThe Mechanism of Wound HealingHanarisha Putri AzkiaNo ratings yet
- ADA Guidelines For Infection Control 3rd EdDocument56 pagesADA Guidelines For Infection Control 3rd Edaprmaster100% (2)
- Communicable Disease Nursing Clinical FocusDocument2 pagesCommunicable Disease Nursing Clinical Focusrceponelas1127No ratings yet
- Colorectal Cancer, How To Diagnosis and TherapyDocument33 pagesColorectal Cancer, How To Diagnosis and TherapyHanarisha Putri AzkiaNo ratings yet
- Faktor Dominan Yang Berhubungan Dengan Kejadian Abortus Imminens Hamidah, Siti MasitohDocument1 pageFaktor Dominan Yang Berhubungan Dengan Kejadian Abortus Imminens Hamidah, Siti MasitohHanarisha Putri AzkiaNo ratings yet
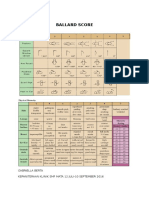
- Ballard Score: Gabriella Berta Kepaniteraan Klinik SMF Mata 12 Juli-10 September 2016Document1 pageBallard Score: Gabriella Berta Kepaniteraan Klinik SMF Mata 12 Juli-10 September 2016Hanarisha Putri AzkiaNo ratings yet
- SMF Anak Rsud Jend. A. Yani Metro Kepaniteraan Klinik FK Unila 2017Document1 pageSMF Anak Rsud Jend. A. Yani Metro Kepaniteraan Klinik FK Unila 2017Hanarisha Putri AzkiaNo ratings yet
- Asymptomatic Bacteriuria in Adults: (E.g., P. Aeruginosa) - Enterococcus Species andDocument6 pagesAsymptomatic Bacteriuria in Adults: (E.g., P. Aeruginosa) - Enterococcus Species andHanarisha Putri AzkiaNo ratings yet
- 2.5 Assesment of Diabetic Foot UlcerDocument10 pages2.5 Assesment of Diabetic Foot UlcerHanarisha Putri AzkiaNo ratings yet
- Anencephaly: A 3 Years Study: DR - Aruna.Eslavath (MD), Dr. Ranga Rao - Diddi (MD), DR - Kalyan Chakravarthy - Valabhaneni (MD)Document4 pagesAnencephaly: A 3 Years Study: DR - Aruna.Eslavath (MD), Dr. Ranga Rao - Diddi (MD), DR - Kalyan Chakravarthy - Valabhaneni (MD)Hanarisha Putri AzkiaNo ratings yet
- Dapus BaruDocument1 pageDapus BaruHanarisha Putri AzkiaNo ratings yet
- ABCs Skin and Wound CareDocument2 pagesABCs Skin and Wound CareHanarisha Putri AzkiaNo ratings yet
- Types of WoundsDocument4 pagesTypes of WoundsHanarisha Putri AzkiaNo ratings yet
- Hyatt 2007 BrainGymDocument9 pagesHyatt 2007 BrainGymmasterbaldomero2012No ratings yet
- Asymptomatic BacteriuriaDocument12 pagesAsymptomatic BacteriuriaNanna de VengerbergNo ratings yet
- Tropical AlmondDocument9 pagesTropical AlmondHanarisha Putri AzkiaNo ratings yet
- Journal of Diagnostic Medical Sonography 2010 Moore 286 9Document4 pagesJournal of Diagnostic Medical Sonography 2010 Moore 286 9Hanarisha Putri AzkiaNo ratings yet
- Nama:Liah Rutama Npm:1343033004 Mata Kuliah:Bahasa Inggris Dosen: Drs - HuzairinDocument4 pagesNama:Liah Rutama Npm:1343033004 Mata Kuliah:Bahasa Inggris Dosen: Drs - HuzairinHanarisha Putri AzkiaNo ratings yet
- Kugel PDFDocument260 pagesKugel PDFUsman SanaNo ratings yet
- Imran Ahmad Sajid-Medical Social Work in Lady Reading Hospital, Peshawar, PakistanDocument52 pagesImran Ahmad Sajid-Medical Social Work in Lady Reading Hospital, Peshawar, PakistanimranahmadsajidNo ratings yet
- Deborah Bartz, M.D. Massachusetts Reprimand On ProfileDocument2 pagesDeborah Bartz, M.D. Massachusetts Reprimand On ProfileAnonymous 8m05a5No ratings yet
- DyalisisDocument24 pagesDyalisisAbdulla Abu EidNo ratings yet
- Alendronate SodiumDocument3 pagesAlendronate SodiumGLen Caniedo100% (1)
- What Is Medical Marijuana?Document8 pagesWhat Is Medical Marijuana?Dragoș TiculaNo ratings yet
- Case Presentation: Alcoholic GastritisDocument18 pagesCase Presentation: Alcoholic Gastritisstancy thomas100% (1)
- Acute Respiratory Distress Syndrome (ARDS)Document3 pagesAcute Respiratory Distress Syndrome (ARDS)akish4uNo ratings yet
- Introduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologyDocument26 pagesIntroduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologymochkurniawanNo ratings yet
- Fissure Treatment in MumbaiDocument4 pagesFissure Treatment in MumbaiSambit ClinicNo ratings yet
- The Valley Gazette - 9.1.11Document14 pagesThe Valley Gazette - 9.1.11Hersam AcornNo ratings yet
- Dematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarDocument1 pageDematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarabhishekNo ratings yet
- The Auburn Plainsman 12-3-1998Document32 pagesThe Auburn Plainsman 12-3-1998The Auburn PlainsmanNo ratings yet
- Dose MonitoringDocument60 pagesDose MonitoringNovan HartantoNo ratings yet
- Gender Differences in Human Brain A Review PDFDocument20 pagesGender Differences in Human Brain A Review PDFSwami GurunandNo ratings yet
- Prenatal Care: Ocampo, Joan Oh, Howard Panganiban, JamesDocument21 pagesPrenatal Care: Ocampo, Joan Oh, Howard Panganiban, JamesHoward Vince OhNo ratings yet
- 4001 EconDocument31 pages4001 EconAngus LeungNo ratings yet
- GSRC Trans Resource Guide (2015-2016)Document19 pagesGSRC Trans Resource Guide (2015-2016)Merissa Taylor-Meissner100% (1)
- 405 Genetics of DementiaDocument12 pages405 Genetics of DementiaLulu LuwiiNo ratings yet
- Peanut Ball Packet Premier Birth ToolsDocument16 pagesPeanut Ball Packet Premier Birth ToolsMar FarréNo ratings yet
- 2 Efast PDFDocument23 pages2 Efast PDFarvinius mariusNo ratings yet