You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Newborn ScreeningDocument20 pagesNewborn ScreeningAlec AnonNo ratings yet
- Laboratory Diagnosis of Viral InfectionDocument35 pagesLaboratory Diagnosis of Viral InfectionHairul Anuar83% (18)
- Nrs 110 Lecture 1 Care Plan WorkshopDocument45 pagesNrs 110 Lecture 1 Care Plan Workshopalphabennydelta4468100% (2)
- Anafilaqsiis Diagnostika Da MartvaDocument8 pagesAnafilaqsiis Diagnostika Da Martvatbilisilovesyou100% (1)
- ADA Medications PDFDocument24 pagesADA Medications PDFRoshni GehlotNo ratings yet
- Heart Rate, Life Expectancy and The Cardiovascular System: Therapeutic ConsiderationsDocument14 pagesHeart Rate, Life Expectancy and The Cardiovascular System: Therapeutic ConsiderationsTapan Kumar RoyNo ratings yet
- Pharma - Safe Dosage Preparation and Drug AdministrationDocument34 pagesPharma - Safe Dosage Preparation and Drug AdministrationVon Javier GamateroNo ratings yet
- Tachycardia Complicated by Bradycardia Then Another Form of TachycardiaDocument7 pagesTachycardia Complicated by Bradycardia Then Another Form of TachycardiaLam Sin WingNo ratings yet
- Cardiology Thesis TopicsDocument4 pagesCardiology Thesis Topicsheatherbjugandesmoines100% (1)
- Curs Postuniv Reconstructie SiniDocument82 pagesCurs Postuniv Reconstructie Sinithanos bakourasNo ratings yet
- Food PoisoningDocument4 pagesFood PoisoningzahidNo ratings yet
- Anaesthesia On The Move PDFDocument256 pagesAnaesthesia On The Move PDFSanna Huhtamaki100% (1)
- History Taking TemplateDocument5 pagesHistory Taking TemplateFatin Nurina Mohd NazemiNo ratings yet
- CasesDocument37 pagesCasesZakaria FarahNo ratings yet
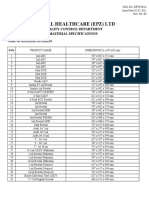
- Revital Healthcare (Epz) LTD: Quality Control Department Material SpecificationsDocument2 pagesRevital Healthcare (Epz) LTD: Quality Control Department Material SpecificationsMusyoka UrbanusNo ratings yet
- Perioperative Nursing Version 2Document38 pagesPerioperative Nursing Version 2Justine CagatanNo ratings yet
- Congenital GlaucomaDocument27 pagesCongenital Glaucomaanon_373532435No ratings yet
- Articulo Fono PDFDocument11 pagesArticulo Fono PDFPaola MartinezNo ratings yet
- Male Pelvic Floor - Advanced Massage and BodyworkDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodyworkpujarze2No ratings yet
- Surgical Vs Non-Surgical Approach in PeriodonticsDocument13 pagesSurgical Vs Non-Surgical Approach in PeriodonticsBea DominguezNo ratings yet
- CANATOY, Charlene S. RES 1 - Thesis 1 Bsstat-3A Ms. Thea C. Galos Assignment 1 - Week 1Document5 pagesCANATOY, Charlene S. RES 1 - Thesis 1 Bsstat-3A Ms. Thea C. Galos Assignment 1 - Week 1Charlene CanatoyNo ratings yet
- Chapter 16Document3 pagesChapter 16RHOSEMARIE AHNN GANDALLANo ratings yet
- Scandinavian PDFDocument2 pagesScandinavian PDFMeghantari PutryNo ratings yet
- Presentation-on-Long-Case (Retinal Detachment)Document33 pagesPresentation-on-Long-Case (Retinal Detachment)Niloy Basak100% (1)
- Frequency and Types of Uterine Anomalies During Caesarean SectionDocument5 pagesFrequency and Types of Uterine Anomalies During Caesarean SectionBOONo ratings yet
- Urinary Tract Infection - FinalDocument86 pagesUrinary Tract Infection - FinalShreyance Parakh100% (1)
- Taylor GLN CH 31Document4 pagesTaylor GLN CH 31Karen Mae AlcantaraNo ratings yet
- Role of Nurse-Non Communicable DiseasesDocument105 pagesRole of Nurse-Non Communicable DiseasesKrishnaveni MurugeshNo ratings yet
- USMLE Step 1 PlanDocument4 pagesUSMLE Step 1 Plansunlight_84100% (2)