You might also like
- Articulo 3Document12 pagesArticulo 3Andrea OrtizNo ratings yet
- Cardiovascular System DiseaseDocument27 pagesCardiovascular System DiseasemarestelbaguiocajesNo ratings yet
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Atrial Utter: 2 PathophysiologyDocument4 pagesAtrial Utter: 2 PathophysiologyZiedTrikiNo ratings yet
- Orthostatic Hypotension in Older AdultsFrom EverandOrthostatic Hypotension in Older AdultsAhmet Turan IsikNo ratings yet
- Heart FailureDocument29 pagesHeart Failuremerin sunilNo ratings yet
- Pulse PressureDocument7 pagesPulse PressureChrisNo ratings yet
- Fisiopatología Shock 1980Document12 pagesFisiopatología Shock 1980Alejo ZubietaNo ratings yet
- 1 A 07 051-062 Unlocked PDFDocument11 pages1 A 07 051-062 Unlocked PDFHarest FauziNo ratings yet
- NCD Lecture-Cardiovascular DisordersDocument133 pagesNCD Lecture-Cardiovascular DisordersYashvi SinghNo ratings yet
- The Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingDocument13 pagesThe Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingFanindya HadamuNo ratings yet
- Meyer2019 HR Dan HFpEFpdfDocument5 pagesMeyer2019 HR Dan HFpEFpdfFaQihuddin AhmadNo ratings yet
- Arterial Stiffness-1Document21 pagesArterial Stiffness-1yoeldp100% (2)
- J of Clinical Hypertension - 2008 - Nichols - Effects of Arterial Stiffness Pulse Wave Velocity and Wave Reflections OnDocument9 pagesJ of Clinical Hypertension - 2008 - Nichols - Effects of Arterial Stiffness Pulse Wave Velocity and Wave Reflections Onizwan taufikNo ratings yet
- Strait 2012Document22 pagesStrait 2012abraham rumayaraNo ratings yet
- Shock and Circulatory FailureDocument8 pagesShock and Circulatory FailureOktaviana Sari DewiNo ratings yet
- Physical Changes With AgingDocument53 pagesPhysical Changes With AgingRohit SejwalNo ratings yet
- NURS 627 Case Study PaperDocument11 pagesNURS 627 Case Study PaperJaclyn Strangie100% (4)
- Physiology & Pathology - Four Common Cardiovascular ConditionsDocument12 pagesPhysiology & Pathology - Four Common Cardiovascular ConditionsAsadNo ratings yet
- Progressive Aortic Stiffness in Aging C57Bl-6 Mice Displays Altered Contractile Behaviour and Extracellular Matrix ChangesDocument11 pagesProgressive Aortic Stiffness in Aging C57Bl-6 Mice Displays Altered Contractile Behaviour and Extracellular Matrix Changesender000No ratings yet
- Cardiac Changes Associated With Vascular Aging: Narayana Sarma V. Singam - Christopher Fine - Jerome L. FlegDocument7 pagesCardiac Changes Associated With Vascular Aging: Narayana Sarma V. Singam - Christopher Fine - Jerome L. Flegabraham rumayaraNo ratings yet
- Inappropiate Sinus TachycardiaDocument9 pagesInappropiate Sinus TachycardiaJazmín Alejandra AGNo ratings yet
- As SNAB Revision NotesDocument49 pagesAs SNAB Revision NotesawinterqueenNo ratings yet
- Cardiovacular SystemDocument44 pagesCardiovacular SystemHimanshuNo ratings yet
- Heart Arteries ArteriolesDocument28 pagesHeart Arteries ArteriolesAndy HermanNo ratings yet
- BradiaritmiaDocument12 pagesBradiaritmiaYolita Satya Gitya UtamiNo ratings yet
- Why Does Atrial Fibrillation Occur?Document38 pagesWhy Does Atrial Fibrillation Occur?khansa nabilaNo ratings yet
- Heart AttackDocument18 pagesHeart AttackKhalifullahNo ratings yet
- PH32 Exp-9qfrDocument2 pagesPH32 Exp-9qfrMello DiaxNo ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- Non-St Segment Elevation Myocardial Infarction (Nstemi)Document24 pagesNon-St Segment Elevation Myocardial Infarction (Nstemi)MHIEMHOINo ratings yet
- S and S: Presenter: Guidance and ModerationDocument60 pagesS and S: Presenter: Guidance and ModerationCatherine PaulNo ratings yet
- Chapter 1 HBPDocument42 pagesChapter 1 HBPmohd ameerNo ratings yet
- The Mechanism of s2 Second Heart Sound Splitting in Normal Physiology and Congenital Heart DefectsDocument4 pagesThe Mechanism of s2 Second Heart Sound Splitting in Normal Physiology and Congenital Heart DefectsSabrinaputri ArrNo ratings yet
- (O. Nelson) Small Animal CardiologyDocument208 pages(O. Nelson) Small Animal CardiologyLoredana Gutu100% (1)
- CMS 251 Unit 1 Cardiovascular SystemDocument114 pagesCMS 251 Unit 1 Cardiovascular SystemAmon RicoNo ratings yet
- Oxen Ham 2003Document9 pagesOxen Ham 2003abraham rumayaraNo ratings yet
- Cheyne-Stokes Respiration in Patients With Heart Failure Prevalence, Causes, Consequences and Treatments - Brack 2012Document12 pagesCheyne-Stokes Respiration in Patients With Heart Failure Prevalence, Causes, Consequences and Treatments - Brack 2012Maxi BoniniNo ratings yet
- Physiological Adaptation of Cardiovascular System To High AltitudeDocument11 pagesPhysiological Adaptation of Cardiovascular System To High AltitudeNicholas Matthew SantosoNo ratings yet
- Collapsing PulseDocument3 pagesCollapsing Pulsemartiqo50% (2)
- Cardiovascular DiseasesDocument6 pagesCardiovascular DiseasesArli MiscalaNo ratings yet
- Homeostasis AssessmentDocument5 pagesHomeostasis AssessmentyrmlarmfarudbisgowNo ratings yet
- 1 s2.0 S0749070421001020 MainDocument12 pages1 s2.0 S0749070421001020 MainEliseu AmaralNo ratings yet
- Cardiovascular SystemDocument16 pagesCardiovascular SystemLinh LeNo ratings yet
- Aging Changes in Cardiovascular SystemDocument7 pagesAging Changes in Cardiovascular SystemVicentenestorg Leh100% (1)
- CV in ElderlyDocument6 pagesCV in ElderlySeli MandianganNo ratings yet
- 01 - Levine - HR & Life ExpectancyDocument3 pages01 - Levine - HR & Life ExpectancyJonathan Ian ArinsolNo ratings yet
- ICCI PatofisiologíaDocument10 pagesICCI PatofisiologíaAndrea Roman chavezNo ratings yet
- ECG HRV Assignment 19334107Document18 pagesECG HRV Assignment 19334107katehughes332No ratings yet
- Heart Health: Week 3 SupplementDocument7 pagesHeart Health: Week 3 Supplementan7li721No ratings yet
- Porth2014 Apa 2018 Disorder of Blood Pressure RegulationDocument27 pagesPorth2014 Apa 2018 Disorder of Blood Pressure RegulationMumtaz MaulanaNo ratings yet
- Chicken Cardiac FailureDocument7 pagesChicken Cardiac FailureSohaib AslamNo ratings yet
- Pe 1 Lesson 2 Non-Communicable DiseasesDocument79 pagesPe 1 Lesson 2 Non-Communicable Diseasesdario serranoNo ratings yet
- Practical of Arterial Pulse For 1st Year Mbbs StudentsDocument7 pagesPractical of Arterial Pulse For 1st Year Mbbs StudentsMudassar Roomi0% (2)
- Cardio Consolidation Notes: MEDS 230: CirculationDocument94 pagesCardio Consolidation Notes: MEDS 230: CirculationtgalksjflkjNo ratings yet
- HypertensionDocument10 pagesHypertensionagus fetal mein feraldNo ratings yet
- 2008 2 92 PDFDocument8 pages2008 2 92 PDFdidiNo ratings yet
- 12015exr PDFDocument10 pages12015exr PDFWahidur Rahman RafsanNo ratings yet
- Respiratory & Circulatory System Regents QuestionsDocument10 pagesRespiratory & Circulatory System Regents Questionsabisantiago613140% (5)
- Buku Panduan ACLS Perki Cetakan 2021 - Hal 11Document1 pageBuku Panduan ACLS Perki Cetakan 2021 - Hal 11yandriasNo ratings yet
- The Diagnosis and Treatment of Pulmonary Valve SteDocument6 pagesThe Diagnosis and Treatment of Pulmonary Valve SteNiarti Ulan SariNo ratings yet
- HPNDocument4 pagesHPNFlorianne AdlawanNo ratings yet
- The Heart - Print - QuizizzDocument5 pagesThe Heart - Print - Quizizzosama100% (1)
- Stroke PreventionDocument3 pagesStroke Preventionapi-27015740100% (2)
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- Nervous Regulation of The Circulation and Rapid Control of Arterial PressureDocument2 pagesNervous Regulation of The Circulation and Rapid Control of Arterial Pressuremcwnotes100% (2)
- NCP Draft XXDocument3 pagesNCP Draft XXTinNo ratings yet
- The ACM v2.0 International PDFDocument76 pagesThe ACM v2.0 International PDFTiago SilvaNo ratings yet
- Handbookofimv 6Document346 pagesHandbookofimv 6Matty LiuNo ratings yet
- Introduction To The CvsDocument43 pagesIntroduction To The CvsParmesh PandeyNo ratings yet
- Antiarrhythmic Drugs - AMBOSS TWO PDFDocument6 pagesAntiarrhythmic Drugs - AMBOSS TWO PDFRuva Oscass JimmyNo ratings yet
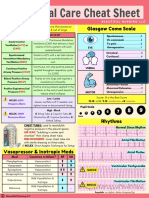
- Critical Care Cheat Sheet FreebieDocument2 pagesCritical Care Cheat Sheet FreebieJeshan Yanong Beltran100% (1)
- BMJ - Hypovolemic ShockDocument5 pagesBMJ - Hypovolemic ShockSamer Darwiche Yasiin100% (1)
- Assessing Heart and Central VesselsDocument34 pagesAssessing Heart and Central VesselsGemmalene Pacleb100% (1)
- The Heart: Test I: Read and Understand The Question Circle The Best AnswerDocument2 pagesThe Heart: Test I: Read and Understand The Question Circle The Best AnswerHolly May MontejoNo ratings yet
- SEMPRO Bismillah PDFDocument15 pagesSEMPRO Bismillah PDFAlisantoniNo ratings yet
- Hypoplastic Left Heart SyndromeDocument26 pagesHypoplastic Left Heart SyndromeKhaled S. HarbNo ratings yet
- ACLS Drugs&Drips Final PDFDocument6 pagesACLS Drugs&Drips Final PDFmesrianti_rubenNo ratings yet
- Deep Vein Thrombosis FlyerDocument2 pagesDeep Vein Thrombosis FlyerMuhammad Reza Syahli PiliangNo ratings yet
- Chapter 3: Lymphatic SystemDocument22 pagesChapter 3: Lymphatic Systemfatin harrisNo ratings yet
- Aritmia AHA 2017Document120 pagesAritmia AHA 2017Corticosteroids MobileLegendNo ratings yet
- ECG NotesDocument8 pagesECG NotesPeer TutorNo ratings yet
- Laporan Kasus Kardio CHF Ec CADDocument35 pagesLaporan Kasus Kardio CHF Ec CADpun212No ratings yet
- Apex Beat..how To LocateDocument20 pagesApex Beat..how To LocateMaha MukhtarNo ratings yet
- Extracorporeal Life Ort Ecls Product CatalogDocument28 pagesExtracorporeal Life Ort Ecls Product CatalogXavi AnpiNo ratings yet
- Color Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IDocument199 pagesColor Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IGorka AguirreNo ratings yet
- ECG Interpretation - Axis and Conduction AbnormalitiesDocument9 pagesECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- Ebook Ekg Plain and Simple 4Th Edition Ellis Test Bank Full Chapter PDFDocument30 pagesEbook Ekg Plain and Simple 4Th Edition Ellis Test Bank Full Chapter PDFalexandercampbelldkcnzafgtw100% (8)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo ratings yet
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (26)