You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
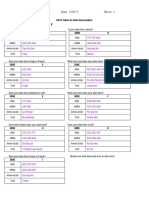
- Data Tables For Alien Gene AnalysisDocument3 pagesData Tables For Alien Gene Analysisapi-382372564100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Exampro A-Level Biology: 3.5.7 - Gene ExpressionDocument16 pagesExampro A-Level Biology: 3.5.7 - Gene Expressionwaheed aluNo ratings yet
- Practical 5: ENZYMES AND DIGESTIONDocument12 pagesPractical 5: ENZYMES AND DIGESTIONhafizah_9071% (7)
- Vaksin Influenza OverviewDocument27 pagesVaksin Influenza OverviewMaria Astika DewiNo ratings yet
- Karolin Luger - Nucleosomes: Structure and FunctionDocument8 pagesKarolin Luger - Nucleosomes: Structure and FunctionDopameNo ratings yet
- Sample & Assay TechnologiesDocument4 pagesSample & Assay Technologieskeven319hk4304No ratings yet
- Aa 1Document39 pagesAa 1Girum SolomonNo ratings yet
- The Forbidden QuestionsDocument30 pagesThe Forbidden QuestionsSivashamugam100% (1)
- Article-2021-COVID-19-Neutralizing Antibodies Predict Disease Severity and SurvivalDocument25 pagesArticle-2021-COVID-19-Neutralizing Antibodies Predict Disease Severity and Survivalcarlos ArozamenaNo ratings yet
- 2018 - 19 20180705145828-Biotechnologyelective PDFDocument19 pages2018 - 19 20180705145828-Biotechnologyelective PDFHarpreet KaurNo ratings yet
- Science 9th Chapter 5 Cell Biology NotesDocument4 pagesScience 9th Chapter 5 Cell Biology NotesavanishNo ratings yet
- SATHYABAMADocument12 pagesSATHYABAMARitesh VeeraniNo ratings yet
- Photosynthesis Review WorksheetDocument9 pagesPhotosynthesis Review Worksheetbrianjay.codillaNo ratings yet
- A Cell Is Like A CompanyDocument1 pageA Cell Is Like A CompanyFRANZ JOSEPH PINEDA HENo ratings yet
- American Society of Plant Biologists (ASPB) The Plant CellDocument6 pagesAmerican Society of Plant Biologists (ASPB) The Plant CellvodounnouNo ratings yet
- Tutorial For MBBS InsulinDocument49 pagesTutorial For MBBS Insulinuzzal ahmedNo ratings yet
- Department of Education: Corresponding Microscope Image by Checking The Column Before ItDocument3 pagesDepartment of Education: Corresponding Microscope Image by Checking The Column Before ItLuz Marie CorveraNo ratings yet
- ClaseDocument7 pagesClasef.tellelopezNo ratings yet
- USF Genetics Unit 4 Exam ReviewDocument3 pagesUSF Genetics Unit 4 Exam ReviewEmma DanelloNo ratings yet
- CAPE 1 Biology - Genetic EngineeringDocument80 pagesCAPE 1 Biology - Genetic EngineeringTamicka BonnickNo ratings yet
- Hopkins Bab 8Document22 pagesHopkins Bab 8ena miladaNo ratings yet
- Valo Health - Pitchdeck - March 2021Document21 pagesValo Health - Pitchdeck - March 2021Rattanan WanikornNo ratings yet
- Cell MembraneDocument24 pagesCell Membraneapi-3733156No ratings yet
- Postlab Protein ConcnDocument25 pagesPostlab Protein ConcnMarie Elexis P. RevillezaNo ratings yet
- Sulphur and The Human BodyDocument1 pageSulphur and The Human BodyAbhijeet BhangeNo ratings yet
- Final Exam ReviewerDocument26 pagesFinal Exam ReviewerRussel Adriane Christian RiveraNo ratings yet
- 30 Reasons To Drink Ningxia Red-HealthyandbrightDocument2 pages30 Reasons To Drink Ningxia Red-HealthyandbrightManfred Lee100% (1)
- Biomolecule & Polymer - Exercise (E)Document19 pagesBiomolecule & Polymer - Exercise (E)aleena'No ratings yet
- Arellano University: Physical ScienceDocument22 pagesArellano University: Physical ScienceMa Angelica MasangcayNo ratings yet
- VCNX PatentDocument36 pagesVCNX PatentCharles GrossNo ratings yet