You might also like
- DTC Codes Mercedes CPC4 EnglishDocument24 pagesDTC Codes Mercedes CPC4 Englishjonny david martinez perez100% (1)
- Perioperative Analgesia After Intrathecal Fentanyl and Morphine or Morphine Alone For Cesarean Section A Randomized Controlled StudyDocument11 pagesPerioperative Analgesia After Intrathecal Fentanyl and Morphine or Morphine Alone For Cesarean Section A Randomized Controlled Studyboby abdul rahmanNo ratings yet
- Adjuvant Agents in Neuraxial Blockade Anaesthesia Tutorial of The Week 230 4 JULY 2011Document10 pagesAdjuvant Agents in Neuraxial Blockade Anaesthesia Tutorial of The Week 230 4 JULY 2011Ifar Irianto YudhowibowoNo ratings yet
- Intravenous Non-Opioid Analgesia For Peri-And Postoperative Pain Management: A Scientific Review of Intravenous Acetaminophen and IbuprofenDocument11 pagesIntravenous Non-Opioid Analgesia For Peri-And Postoperative Pain Management: A Scientific Review of Intravenous Acetaminophen and IbuprofenUmy PolpokeNo ratings yet
- Adjuvant Neuroaxial BlokDocument12 pagesAdjuvant Neuroaxial BlokDadanaja AjaNo ratings yet
- Management of Postoperative Pain: Anaesthesia SupplementDocument4 pagesManagement of Postoperative Pain: Anaesthesia SupplementBani ZakiyahNo ratings yet
- Dexmedetomidine or Fentanyl, Which One Is Better As An Adjunct Drug in Epidural Anesthesia and Causes More Postoperative Pain ReductionDocument8 pagesDexmedetomidine or Fentanyl, Which One Is Better As An Adjunct Drug in Epidural Anesthesia and Causes More Postoperative Pain Reductionzidni fatayanNo ratings yet
- Effective Methods for Labour AnalgesiaDocument11 pagesEffective Methods for Labour AnalgesiaAriefNo ratings yet
- Intrathecal MorphineDocument6 pagesIntrathecal MorphineJoana MoreiraNo ratings yet
- Morfina IT. Dosis Bajas en HTADocument8 pagesMorfina IT. Dosis Bajas en HTAChurrunchaNo ratings yet
- Obat AnastesiDocument10 pagesObat AnastesiIndah Rian PuspitasariNo ratings yet
- Medications For Analgesia and Sedation in The Intensive Care Unit: An OverviewDocument5 pagesMedications For Analgesia and Sedation in The Intensive Care Unit: An OverviewJohn MaynhamNo ratings yet
- Medicamentos Sedacion UCI PDFDocument5 pagesMedicamentos Sedacion UCI PDFAnnison Hector Ramos BravoNo ratings yet
- M. MorganDocument24 pagesM. MorgansufealNo ratings yet
- Httpsscielo Isciii Espdfdolorv19n2revisionmbe PDFDocument23 pagesHttpsscielo Isciii Espdfdolorv19n2revisionmbe PDFJoelGámezNo ratings yet
- 8a. General AnaesthesiaDocument28 pages8a. General Anaesthesiamatchees-gone rogueNo ratings yet
- Amalia 163216 - Journal ReadingDocument26 pagesAmalia 163216 - Journal ReadingGhifari FarandiNo ratings yet
- Perioperative Uses of Intravenous Opioids in Adults - General Considerations - UpToDateDocument32 pagesPerioperative Uses of Intravenous Opioids in Adults - General Considerations - UpToDatemayteveronica1000No ratings yet
- Journal Course Evidence Based Use of Nonopioid Analgesics August 2018Document7 pagesJournal Course Evidence Based Use of Nonopioid Analgesics August 2018DesywinNo ratings yet
- Monitored Anesthesia Care An OverviewDocument3 pagesMonitored Anesthesia Care An OverviewLestari Chye PouedanNo ratings yet
- Notas de Analgesia en EmbarazadasDocument7 pagesNotas de Analgesia en EmbarazadasRicardo LunaNo ratings yet
- Wja 3 191Document13 pagesWja 3 191mikayNo ratings yet
- Scandinavian Journal of Pain: Harald BreivikDocument2 pagesScandinavian Journal of Pain: Harald BreivikdianNo ratings yet
- General Anaesthesia: Anaesthesia and Critical Care DeptDocument46 pagesGeneral Anaesthesia: Anaesthesia and Critical Care DeptAnonymous A2d5hUNeMiNo ratings yet
- DR Amutha DR Manjit DR Priyanka DR SubratoDocument37 pagesDR Amutha DR Manjit DR Priyanka DR SubratoParvathy R NairNo ratings yet
- Approach To The Patient With Postoperative PainDocument15 pagesApproach To The Patient With Postoperative PainbarbarabarbarabarbaraNo ratings yet
- Treatment Without OpioidesDocument20 pagesTreatment Without OpioidesDanii LaverdeNo ratings yet
- Psychology of Labour PainDocument6 pagesPsychology of Labour PainJohara MacasindelNo ratings yet
- Anaesthesia - 2021 - Sultan - Regional Anaesthesia For Labour Operative Vaginal Delivery and Caesarean Delivery ADocument12 pagesAnaesthesia - 2021 - Sultan - Regional Anaesthesia For Labour Operative Vaginal Delivery and Caesarean Delivery Aeralp cevikkalpNo ratings yet
- A Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesDocument16 pagesA Comparative Study of Intrathecal Injection of Bupivacaine Alone or With Fentanyl, Clonidine, and Neostigmine in Lower Abdominal SurgeriesdhiyaNo ratings yet
- Fisiologia de Los Opioides Epidurales e IntratectalesDocument13 pagesFisiologia de Los Opioides Epidurales e Intratectalessanjuandediosanestesia100% (5)
- Opioid-Free AnesthesiaDocument8 pagesOpioid-Free AnesthesiaPaulina LugoNo ratings yet
- Opioid-Free Anaesthesia - Atow-461-00 - BDocument6 pagesOpioid-Free Anaesthesia - Atow-461-00 - BEugenio Martinez HurtadoNo ratings yet
- PROTOCOL - RASEL (1st Review)Document35 pagesPROTOCOL - RASEL (1st Review)habibbuetNo ratings yet
- New options for managing pain after caesarean sectionsDocument4 pagesNew options for managing pain after caesarean sectionsnaufal12345No ratings yet
- Natural Opioids Vs Synthetic Opioids As Adjuvant in Regional AnesthesiaDocument21 pagesNatural Opioids Vs Synthetic Opioids As Adjuvant in Regional AnesthesiaSyamsuriWahyuNo ratings yet
- General Anaesthesia: Understanding the ProcessDocument8 pagesGeneral Anaesthesia: Understanding the ProcessJugal AryaNo ratings yet
- Acute and Chronic Pain Following CraniotomyDocument7 pagesAcute and Chronic Pain Following CraniotomyLusy Octavia SaputriNo ratings yet
- DwefgnmjDocument8 pagesDwefgnmjfabian arassiNo ratings yet
- Postoperative Analgesia in Neonates and ChildrenDocument200 pagesPostoperative Analgesia in Neonates and Childrenkhumaira1982No ratings yet
- Indications and Outcomes of Nefopam Administration in Palliative Care PatientsDocument15 pagesIndications and Outcomes of Nefopam Administration in Palliative Care PatientsHamsa veniNo ratings yet
- Sultana OFADocument7 pagesSultana OFANurshadrinaHendrakaraminaNo ratings yet
- Ijca 7 2 313 318Document6 pagesIjca 7 2 313 318Bianca CaterinalisendraNo ratings yet
- Case Study PropofolDocument7 pagesCase Study PropofolaliasLiew100% (1)
- Perioperative Pain Management in Colorectal Surgery: Vinay Ratnalikar Catrin Williams Thomas MosesDocument7 pagesPerioperative Pain Management in Colorectal Surgery: Vinay Ratnalikar Catrin Williams Thomas Mosesdian lukman hakimNo ratings yet
- Post CraniotomyDocument10 pagesPost CraniotomyTika HandayaniNo ratings yet
- Intrathecal Clonidine As Spinal Anaesthesia AdjuvantDocument26 pagesIntrathecal Clonidine As Spinal Anaesthesia Adjuvantlaksoburgo3No ratings yet
- 15-Kip Aaanalgesia Under AnaesthesiaDocument13 pages15-Kip Aaanalgesia Under AnaesthesiagospelcorpNo ratings yet
- NIH Public Access: Effect of Sedation On Pain PerceptionDocument21 pagesNIH Public Access: Effect of Sedation On Pain PerceptionAgustina ZairidaNo ratings yet
- IV PCDocument27 pagesIV PCNusrat Jahan MuniaNo ratings yet
- Management of Chronic Pain in The Elderly: Focus On Transdermal BuprenorphineDocument10 pagesManagement of Chronic Pain in The Elderly: Focus On Transdermal BuprenorphineancoursNo ratings yet
- Fiebre en El Lactante y Nino PequenoDocument6 pagesFiebre en El Lactante y Nino Pequenoalberto mendozaNo ratings yet
- Anesthetic Drugs Jonathan Bland Pathophysiology Professor Lori McgowanDocument4 pagesAnesthetic Drugs Jonathan Bland Pathophysiology Professor Lori McgowanjonNo ratings yet
- Fentanyl, Also Spelled Fentanil, Is An: o o o o o o o o oDocument3 pagesFentanyl, Also Spelled Fentanil, Is An: o o o o o o o o oChristian ConsignaNo ratings yet
- SP Ade NurkacanDocument7 pagesSP Ade NurkacanHidayati IdaNo ratings yet
- Fundamentals and Innovations in Regional Anaesthesia For Infants and ChildrenDocument15 pagesFundamentals and Innovations in Regional Anaesthesia For Infants and ChildrenLuisArroboNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument29 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNi Putu Ari FebriantariNo ratings yet
- Peripheral Interventional Management in HeadacheFrom EverandPeripheral Interventional Management in HeadacheAynur ÖzgeNo ratings yet
- Handbook of Methadone Prescribing and Buprenorphine TherapyFrom EverandHandbook of Methadone Prescribing and Buprenorphine TherapyNo ratings yet
- Aspiration of Breast Abscess Through Wide Bore 14-Gauge Intravenous CannulaDocument3 pagesAspiration of Breast Abscess Through Wide Bore 14-Gauge Intravenous CannulaPalwasha MalikNo ratings yet
- Psychosocial Concerns Station PDFDocument2 pagesPsychosocial Concerns Station PDFPalwasha MalikNo ratings yet
- ps52 2015 Guidelines For Transport of Critically Ill Patients PDFDocument12 pagesps52 2015 Guidelines For Transport of Critically Ill Patients PDFPalwasha MalikNo ratings yet
- Psychosocial Concerns Station PDFDocument2 pagesPsychosocial Concerns Station PDFPalwasha MalikNo ratings yet
- Presenting ExaminationsDocument1 pagePresenting ExaminationsPalwasha MalikNo ratings yet
- Diebetic Foot FinalDocument27 pagesDiebetic Foot FinalPalwasha MalikNo ratings yet
- Pod 2166545286Document1 pagePod 2166545286Palwasha MalikNo ratings yet
- College of Physicians & Surgeons Pakistan: Online Application Form For FCPS-II (MAJOR SUBJECTS)Document3 pagesCollege of Physicians & Surgeons Pakistan: Online Application Form For FCPS-II (MAJOR SUBJECTS)Palwasha MalikNo ratings yet
- ps52 2015 Guidelines For Transport of Critically Ill Patients PDFDocument12 pagesps52 2015 Guidelines For Transport of Critically Ill Patients PDFPalwasha MalikNo ratings yet
- Pakistan Repeater PDFDocument1 pagePakistan Repeater PDFPalwasha MalikNo ratings yet
- Inquiry Mukhtiar AliDocument2 pagesInquiry Mukhtiar AliPalwasha MalikNo ratings yet
- E-Tag Application FormDocument2 pagesE-Tag Application FormPalwasha MalikNo ratings yet
- ViewDocument6 pagesViewPalwasha MalikNo ratings yet
- Aspiration of Breast Abscess Through Wide Bore 14-Gauge Intravenous CannulaDocument3 pagesAspiration of Breast Abscess Through Wide Bore 14-Gauge Intravenous CannulaPalwasha MalikNo ratings yet
- Cqhhe1GB PDFDocument6 pagesCqhhe1GB PDFPalwasha MalikNo ratings yet
- MRCS Part A Change NoticeDocument1 pageMRCS Part A Change NoticePalwasha MalikNo ratings yet
- ClarificationsDocument3 pagesClarificationsPalwasha MalikNo ratings yet
- JhUUjgTO PDFDocument51 pagesJhUUjgTO PDFPalwasha MalikNo ratings yet
- Blue RegulationsDocument10 pagesBlue RegulationsPalwasha MalikNo ratings yet
- Regulations For The Intercollegiate Membership Examination of The Surgical Royal Colleges of Great Britain and in IrelandDocument10 pagesRegulations For The Intercollegiate Membership Examination of The Surgical Royal Colleges of Great Britain and in IrelandPalwasha MalikNo ratings yet
- MRCS PART B OSCE APPLICATION SINGAPOREDocument6 pagesMRCS PART B OSCE APPLICATION SINGAPOREPalwasha MalikNo ratings yet
- CT in Small Bowel ObstDocument5 pagesCT in Small Bowel ObstPalwasha MalikNo ratings yet
- Title PageDocument2 pagesTitle PagePalwasha MalikNo ratings yet
- CT in Small Bowel Obst PDFDocument23 pagesCT in Small Bowel Obst PDFPalwasha MalikNo ratings yet
- Mortality RepoortDocument8 pagesMortality RepoortPalwasha MalikNo ratings yet
- Table 1: Results of All PatientsDocument2 pagesTable 1: Results of All PatientsPalwasha MalikNo ratings yet
- 05 Advice To CandidatesDocument2 pages05 Advice To CandidatesbkprosthoNo ratings yet
- Sensitivity of CT Scan in Intestinal Obstruction ArticleDocument3 pagesSensitivity of CT Scan in Intestinal Obstruction ArticlePalwasha MalikNo ratings yet
- Shock: Differential Diagnosis and Hemodynamic MonitoringDocument21 pagesShock: Differential Diagnosis and Hemodynamic MonitoringtataranyNo ratings yet
- Morbidity - DR Rizwan Khan 1Document13 pagesMorbidity - DR Rizwan Khan 1Palwasha MalikNo ratings yet
- Mapeh-7pe Q2 Summative-TestDocument2 pagesMapeh-7pe Q2 Summative-TestVhannie AcquiatanNo ratings yet
- WRBS Quarter 1 Modules WEEK-1-8Document32 pagesWRBS Quarter 1 Modules WEEK-1-8Sir Kindred VillaruzNo ratings yet
- Taeka HaileleulDocument167 pagesTaeka HaileleulBini100% (1)
- Company Introduction PT GEADocument8 pagesCompany Introduction PT GEABegawan Half DoneNo ratings yet
- 255 Introduction Vocational Service enDocument12 pages255 Introduction Vocational Service enDmitri PopaNo ratings yet
- Instruction Manual: Shimadzu Analytical BalanceDocument169 pagesInstruction Manual: Shimadzu Analytical BalanceChanthar SoeNo ratings yet
- AET Aetna 2017 Investor Day Presentation - Final (For Website) PDFDocument73 pagesAET Aetna 2017 Investor Day Presentation - Final (For Website) PDFAla BasterNo ratings yet
- Conversion Cycle (Process Cost) : Rizal Technological UniversityDocument25 pagesConversion Cycle (Process Cost) : Rizal Technological UniversityHatdogNo ratings yet
- Astm A710Document3 pagesAstm A710Cristian Otivo100% (1)
- Use of Passive VoiceDocument13 pagesUse of Passive VoiceLuciana DicieroNo ratings yet
- Highway Planning EssentialsDocument106 pagesHighway Planning EssentialsKevin Salzal100% (1)
- 01 A Beginner's Guide To TajikiDocument384 pages01 A Beginner's Guide To Tajikitaryuman100% (1)
- Review Relative Clauses, Articles, and ConditionalsDocument10 pagesReview Relative Clauses, Articles, and ConditionalsNgoc AnhNo ratings yet
- Mason E0010Document24 pagesMason E0010SandeepNo ratings yet
- Vedic Healing Through Gems4Document3 pagesVedic Healing Through Gems4gesNo ratings yet
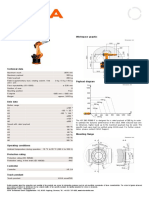
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Probability Concepts and Random Variable - SMTA1402: Unit - IDocument105 pagesProbability Concepts and Random Variable - SMTA1402: Unit - IVigneshwar SNo ratings yet
- Organization-and-Management Q1 LAS Wk1Document5 pagesOrganization-and-Management Q1 LAS Wk1Joyce CelineNo ratings yet
- The Impact of COVID-19 On The Steel IndustryDocument25 pagesThe Impact of COVID-19 On The Steel IndustryAyesha KhalidNo ratings yet
- 2 Corinthians: Workbook OnDocument18 pages2 Corinthians: Workbook OnJhon Ray OtañesNo ratings yet
- Course 1 ProjectDocument6 pagesCourse 1 ProjectDhruvNo ratings yet
- Nature of MarketingDocument15 pagesNature of MarketingMohamaad SihatthNo ratings yet
- Murder Conviction UpheldDocument9 pagesMurder Conviction UpheldBobNo ratings yet
- Is The Sustainable Development Goals (SDG) Index An Adequate Framework To Measure The Progress of The 2030 Agenda?Document9 pagesIs The Sustainable Development Goals (SDG) Index An Adequate Framework To Measure The Progress of The 2030 Agenda?hadi_friendNo ratings yet
- TLC Visualization SolutionsDocument3 pagesTLC Visualization SolutionseraborNo ratings yet
- Of Our TimesDocument84 pagesOf Our TimesThe Journal of Music100% (1)
- Human Ear and Role of Hearing in HCIDocument4 pagesHuman Ear and Role of Hearing in HCIrafia0% (1)
- Employee Leave Management System: FUDMA Journal of Sciences July 2020Document7 pagesEmployee Leave Management System: FUDMA Journal of Sciences July 2020MOHAMMED ASHICKNo ratings yet
- Acid-Base Titration Using PH Meter and Finding The Equivalence Point Naoh ConcentrationDocument8 pagesAcid-Base Titration Using PH Meter and Finding The Equivalence Point Naoh ConcentrationYocobSamandrewsNo ratings yet