You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- BS-200&220&330&350 - Service Manual - V8.0 - ENDocument137 pagesBS-200&220&330&350 - Service Manual - V8.0 - ENLuis OvalleNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case 3 Analysis AdtrackmediaDocument2 pagesCase 3 Analysis Adtrackmediaapi-526105414No ratings yet
- MRP BajajDocument352 pagesMRP BajajRanesh Kumar0% (1)
- Formula B1 Unit 7 Test DFDocument6 pagesFormula B1 Unit 7 Test DFmarxuky21No ratings yet
- SustainabilityDocument856 pagesSustainabilityErnest AcarNo ratings yet
- Speech As A Signal of Social IdentityDocument25 pagesSpeech As A Signal of Social IdentityAysha BahaaNo ratings yet
- Chapter 5-Leadership and MotivationDocument62 pagesChapter 5-Leadership and MotivationAklilu GirmaNo ratings yet
- Hf1016414 Hoffman VentiladorDocument4 pagesHf1016414 Hoffman VentiladorMoises AlvarezNo ratings yet
- Keph205 PDFDocument18 pagesKeph205 PDFRohit Kumar YadavNo ratings yet
- Lecture 14: Nonparametric Survival Analysis Methods: James J. DignamDocument43 pagesLecture 14: Nonparametric Survival Analysis Methods: James J. DignamcdcdiverNo ratings yet
- Government AccountingDocument32 pagesGovernment AccountingLaika Mae D. CariñoNo ratings yet
- The Influence of Wheel-Rail Contact Conditions On The Microstructure and Hardness of Railway WheelsDocument16 pagesThe Influence of Wheel-Rail Contact Conditions On The Microstructure and Hardness of Railway Wheelswwd819No ratings yet
- Drainage Morphology of Imo Basin in The Anambra - Imo River Basin Area, of Imo State, Southern NigeriaDocument11 pagesDrainage Morphology of Imo Basin in The Anambra - Imo River Basin Area, of Imo State, Southern NigeriannekaNo ratings yet
- Scheme of Work Science Stage 9.v1Document51 pagesScheme of Work Science Stage 9.v1Sue Adames de Velasco50% (2)
- 8 - Schlumberger - Alberto Stevens Well Integrity Evaluation With Wireline LogsDocument16 pages8 - Schlumberger - Alberto Stevens Well Integrity Evaluation With Wireline LogsHendrik FoxNo ratings yet
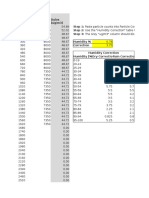
- Dylos Conversion Education - Cehs.health - Umt.eduDocument117 pagesDylos Conversion Education - Cehs.health - Umt.eduMCNo ratings yet
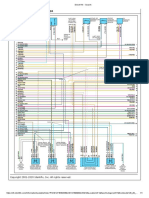
- Diagram 2 Data Link ConnectorDocument1 pageDiagram 2 Data Link ConnectorJoycee Lázaro ReyesNo ratings yet
- Progress of Refractories Used in BFDocument8 pagesProgress of Refractories Used in BFAloísio Simões RibeiroNo ratings yet
- ABB Controls Training Brochure Jul-Dec 2014 PDFDocument4 pagesABB Controls Training Brochure Jul-Dec 2014 PDFpurwantoNo ratings yet
- TissueDocument54 pagesTissueNicole EncinaresNo ratings yet
- Cloudworx Microstation UsDocument2 pagesCloudworx Microstation Usguru4lifegmailcomNo ratings yet
- 7 Revealing Depression Questions Answered: Health - Body - Life - SoulDocument4 pages7 Revealing Depression Questions Answered: Health - Body - Life - SoulGregorio PetteNo ratings yet
- Answer Key-Averages ExerciseDocument3 pagesAnswer Key-Averages ExerciseVanshika WadhwaniNo ratings yet
- Designreport Ner Roads Idg Sep19Document110 pagesDesignreport Ner Roads Idg Sep19yoseph dejeneNo ratings yet
- Case Study of Kaleshwaram ProjectDocument4 pagesCase Study of Kaleshwaram ProjectsujithaNo ratings yet
- Cargo Terminal Standards 121021Document16 pagesCargo Terminal Standards 121021suryakeshwar singhNo ratings yet
- CHM 217 - TartrazineDocument7 pagesCHM 217 - Tartrazineraphaelmohara04No ratings yet
- Machine Learning Classification Model For Identifying Wildlife Species in East AfricaDocument9 pagesMachine Learning Classification Model For Identifying Wildlife Species in East AfricaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mead's Theory of The SelfDocument1 pageMead's Theory of The Selfsumayya tariqNo ratings yet
- Heart Disease and Stroke BrochureDocument3 pagesHeart Disease and Stroke Brochureapi-461951012No ratings yet