You might also like
- Dyspareunia A Difficult Symptom in Gynaecological Practice 2015 Obstetrics Gynaecology Reproductive MedicineDocument6 pagesDyspareunia A Difficult Symptom in Gynaecological Practice 2015 Obstetrics Gynaecology Reproductive MedicineNoraNo ratings yet
- Fensterstock Albert - Credit Scoring and The Next StepDocument4 pagesFensterstock Albert - Credit Scoring and The Next Stephenrique_olivNo ratings yet
- Oman Law For Radioactive MaterialDocument6 pagesOman Law For Radioactive MaterialTabish Shaikh100% (1)
- BioFactura-CBMS VRP ProposalDocument218 pagesBioFactura-CBMS VRP ProposalpabloNo ratings yet
- Novel Drug Delivery Techniques-A Changing and Challenging Global ScenarioDocument15 pagesNovel Drug Delivery Techniques-A Changing and Challenging Global ScenarioARUNKANTH KRISHNAKUMARNo ratings yet
- Cyclotron Radionuclides FDG PDFDocument172 pagesCyclotron Radionuclides FDG PDFMark Denham100% (1)
- QP-022 Sterilization Process ValidationDocument2 pagesQP-022 Sterilization Process Validationesraa asemNo ratings yet
- WHP Isolation GloveIntegrityTesting R1Document2 pagesWHP Isolation GloveIntegrityTesting R1Mina Maher MikhailNo ratings yet
- SuspensionsDocument22 pagesSuspensionsMuhammad AriefNo ratings yet
- Bowie Dick Test Efhss Conf2006 Lecture17 enDocument42 pagesBowie Dick Test Efhss Conf2006 Lecture17 enPrakashKandaswamyNo ratings yet
- Aorn Recomentation Practices PDFDocument15 pagesAorn Recomentation Practices PDFWandi HuseinNo ratings yet
- AdvaMed CAPA GuideDocument26 pagesAdvaMed CAPA GuideOmer ZiaNo ratings yet
- Continued Process VerificationDocument4 pagesContinued Process VerificationAbdul KalimNo ratings yet
- ParisonDocument12 pagesParisonJay KumarNo ratings yet
- HTM0101PartC STERILIZER PDFDocument99 pagesHTM0101PartC STERILIZER PDFLuis CárdenasNo ratings yet
- Gamma IrradiationDocument27 pagesGamma Irradiationmuzammil21_adNo ratings yet
- Water Quality Testing Protocol-WaterAid Pakistan - Final PDFDocument12 pagesWater Quality Testing Protocol-WaterAid Pakistan - Final PDFDani DaniNo ratings yet
- Central Sterile Supply Services Policy KKM PDFDocument53 pagesCentral Sterile Supply Services Policy KKM PDFGerald TalledoNo ratings yet
- Laboratory Biosafety Manual 4ed. - Decontamination and Waste ManagementDocument62 pagesLaboratory Biosafety Manual 4ed. - Decontamination and Waste ManagementSergio RamosNo ratings yet
- Aada: Aao: Ade: Adme: Adi: Adr: Adrs: Agdufa: Ahu: Alcoa: Alcoa PlusDocument10 pagesAada: Aao: Ade: Adme: Adi: Adr: Adrs: Agdufa: Ahu: Alcoa: Alcoa PlusjhansiNo ratings yet
- Quality Assurance Manual: WWW - Penndot.govDocument61 pagesQuality Assurance Manual: WWW - Penndot.govSami AjNo ratings yet
- Medical Sterilization Methods - LemoDocument52 pagesMedical Sterilization Methods - LemoPedro GomesNo ratings yet
- White Paper New Changes To Cleanroom and Clean Air Device ClassificationsDocument8 pagesWhite Paper New Changes To Cleanroom and Clean Air Device ClassificationsjerryNo ratings yet
- 62 The Basics of Bioburden TestingDocument2 pages62 The Basics of Bioburden Testinghitham shehataNo ratings yet
- Aesculap SterilContainer System Instructions For Use SOP-AIC-5001592Document61 pagesAesculap SterilContainer System Instructions For Use SOP-AIC-5001592ludi100% (1)
- Biological Evaluation of Medical Devices / Biosafety: Applicable ProductsDocument5 pagesBiological Evaluation of Medical Devices / Biosafety: Applicable ProductsAnonymous iqoU1mtNo ratings yet
- WHO IVB 14.07 EngDocument14 pagesWHO IVB 14.07 EnggineNo ratings yet
- Multiprobe Temperature Verification Kit 4460108ADocument57 pagesMultiprobe Temperature Verification Kit 4460108APatricia MendozaNo ratings yet
- Reducing Airborne Exposure of COVID 19 Using Air Filtration Systems WhitePaperDocument9 pagesReducing Airborne Exposure of COVID 19 Using Air Filtration Systems WhitePaperColectibondiNo ratings yet
- Tutt E - Tech ManualDocument206 pagesTutt E - Tech ManualDidi HernandezNo ratings yet
- Pharmaceutical ExcipientsDocument5 pagesPharmaceutical Excipientsmads56091No ratings yet
- Process Failures HO RoseDocument14 pagesProcess Failures HO RoseHilario AlinabonNo ratings yet
- WHO Dermal AbsorptionDocument217 pagesWHO Dermal AbsorptionAleponNo ratings yet
- When U Have A Bowie Dick TestDocument6 pagesWhen U Have A Bowie Dick TestboddarambabuNo ratings yet
- Sterilization (Microbiology) : ApplicationsDocument12 pagesSterilization (Microbiology) : ApplicationsChiou HuahNo ratings yet
- Sterlization TechniqueDocument32 pagesSterlization TechniquenehadewasiNo ratings yet
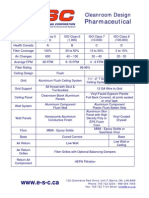
- Cleanroom Design Criteria PharmaceuticalDocument1 pageCleanroom Design Criteria PharmaceuticalNabil RamNo ratings yet
- Leseprobe FundamentalsDocument14 pagesLeseprobe FundamentalsDinesh SenathipathiNo ratings yet
- CleaningDocument3 pagesCleaningKARENMCGUIRK2011100% (1)
- CTD CMC-Information-Human-Gene-Therapy-IND-Applications - Jan - 2020Document56 pagesCTD CMC-Information-Human-Gene-Therapy-IND-Applications - Jan - 2020Shiraz KhanNo ratings yet
- Phuong - DryheatDocument5 pagesPhuong - DryheatqhpuongNo ratings yet
- USFDA Regulatory Toxicology OverviewDocument100 pagesUSFDA Regulatory Toxicology OverviewHarsh KoshtiNo ratings yet
- Cleaning Sanitisation Disinfection Annex1 PDFDocument4 pagesCleaning Sanitisation Disinfection Annex1 PDFAbhiNo ratings yet
- Steam SterilizationDocument2 pagesSteam SterilizationHumayun KhanNo ratings yet
- Class 10000 Iso 7 Cleanroom CleaningDocument5 pagesClass 10000 Iso 7 Cleanroom CleaningRafael De JesusNo ratings yet
- Mecart Brochure PDFDocument20 pagesMecart Brochure PDFShenina KnightleyNo ratings yet
- 2 Understanding Cleanroom Classification PDFDocument22 pages2 Understanding Cleanroom Classification PDFTECHNO DATENo ratings yet
- Ausdiagnostics High-Plex Analyser Maintenance Procedure: 1. Standard Dtprime Maintenance GuideDocument12 pagesAusdiagnostics High-Plex Analyser Maintenance Procedure: 1. Standard Dtprime Maintenance GuideJimNo ratings yet
- The Future of Systems Validation ACF1D6Document3 pagesThe Future of Systems Validation ACF1D6Mitchel JammalNo ratings yet
- NPMA Bed Bug Laws ManualDocument3 pagesNPMA Bed Bug Laws ManualSteven DixonNo ratings yet
- A Global Disinfectant Standard For CleanDocument9 pagesA Global Disinfectant Standard For CleanAyman EshraNo ratings yet
- 320 Other 1210 2 10 20180111Document10 pages320 Other 1210 2 10 20180111Vivek PrasadNo ratings yet
- CSSDDocument35 pagesCSSDAzmi Tok-tokNo ratings yet
- Whole Room DisinfectionDocument68 pagesWhole Room Disinfectionkfujiwar100% (1)
- Microbiological Commissioning and MonitoringDocument28 pagesMicrobiological Commissioning and MonitoringSungkakNo ratings yet
- Urology Overview: Part II: CIS Self-Study Lesson PlanDocument5 pagesUrology Overview: Part II: CIS Self-Study Lesson Planjerimiah_manzonNo ratings yet
- Global Perspectives in Cleaning ValidationDocument17 pagesGlobal Perspectives in Cleaning ValidationYusuf SalahamanaNo ratings yet
- Dyspareunia: Colin Macneill, MDDocument13 pagesDyspareunia: Colin Macneill, MDFELIPE MEDINANo ratings yet
- Vaginal ItchingDocument2 pagesVaginal ItchingHervis Francisco FantiniNo ratings yet
- Samia Batool - 1577-FSS-BSPSY-F20 Psy AssignDocument5 pagesSamia Batool - 1577-FSS-BSPSY-F20 Psy Assignsamiabatool015No ratings yet
- The Sexual Key To The Tarot - Theodor LaurenceDocument129 pagesThe Sexual Key To The Tarot - Theodor LaurenceLola Flores100% (2)
- Abs - DXBD - Male Escort - Dubai, UAE Rent - MenDocument1 pageAbs - DXBD - Male Escort - Dubai, UAE Rent - MensamehNo ratings yet
- Transgender Leadership Conclave BrochureDocument4 pagesTransgender Leadership Conclave BrochureMAYANK CHHATWALNo ratings yet
- Taligaman National High SchoolDocument3 pagesTaligaman National High SchoolMelvin CabonegroNo ratings yet
- The Courage To Heal Workbook A Guide For PDFDocument3 pagesThe Courage To Heal Workbook A Guide For PDFEricka Romero0% (13)
- Guildelines For Hiv Testing NacoDocument165 pagesGuildelines For Hiv Testing NacoNagendra Singh BeniwalNo ratings yet
- Sex Workers Policy 1ac - Wake 2019Document76 pagesSex Workers Policy 1ac - Wake 2019ConnorNo ratings yet
- Four Chord SongDocument8 pagesFour Chord SongAnthony RichardNo ratings yet
- Sex, Love and RomanceDocument28 pagesSex, Love and Romancevain911No ratings yet
- Charting Examples For Physical AssessmentDocument16 pagesCharting Examples For Physical Assessmentim3in1No ratings yet
- 25 Day "Think Sex" Challenge With Sexy CouponsDocument15 pages25 Day "Think Sex" Challenge With Sexy CouponshmareidNo ratings yet
- House Hearing, 114TH Congress - Gendercide: China's Missing GirlsDocument98 pagesHouse Hearing, 114TH Congress - Gendercide: China's Missing GirlsScribd Government DocsNo ratings yet
- Osmundo Pinho-The - Black - Male - Body - and - Sex - Wars - in - Brazil PDFDocument20 pagesOsmundo Pinho-The - Black - Male - Body - and - Sex - Wars - in - Brazil PDFMateo Armando MeloNo ratings yet
- Descriptions of HeatDocument9 pagesDescriptions of HeatanishkrishnannayarNo ratings yet
- Female Genital Mutilation/Cutting: A Statistical Overview and Exploration of The Dynamics of ChangeDocument194 pagesFemale Genital Mutilation/Cutting: A Statistical Overview and Exploration of The Dynamics of ChangeUNICEF100% (1)
- The Word "SQUAW"Document10 pagesThe Word "SQUAW"Frank Waabu O'Brien (Dr. Francis J. O'Brien Jr.)100% (3)
- Freud Personality and ConflictDocument5 pagesFreud Personality and ConflictchaitalideNo ratings yet
- DallowayreasearchandanalysisDocument3 pagesDallowayreasearchandanalysisapi-319753967No ratings yet
- Progesterone in PregnancyDocument59 pagesProgesterone in PregnancyKaruna Indoliya100% (2)
- PC Rob LopicolaDocument9 pagesPC Rob LopicolaSergio Nahuel CandidoNo ratings yet
- Thanda Gosht and Khol Do by Saadat HasanDocument6 pagesThanda Gosht and Khol Do by Saadat HasanKaushik RayNo ratings yet
- 07-15-10 Issue of The San Mateo Daily JournalDocument26 pages07-15-10 Issue of The San Mateo Daily JournalSan Mateo Daily JournalNo ratings yet
- Yet Bed Any For Travelling Assistance Indulgence UnpleasingDocument2 pagesYet Bed Any For Travelling Assistance Indulgence UnpleasingAndie PlayerNo ratings yet
- Criticism, Edited by Arlyn Diamond and Lee R. EdwardsDocument3 pagesCriticism, Edited by Arlyn Diamond and Lee R. EdwardsAlexandra ElenaNo ratings yet
- Emergent Momentum For EqualityDocument17 pagesEmergent Momentum For EqualityJanin GallanaNo ratings yet
- Phylum NematodaDocument285 pagesPhylum NematodaBrielleNo ratings yet
- Homophile MovementDocument14 pagesHomophile Movementapi-404628226100% (1)
- Psychology Assignment APFCC Ha He HO IV DV Ethnics On Internet Addition Article.Document2 pagesPsychology Assignment APFCC Ha He HO IV DV Ethnics On Internet Addition Article.chl23No ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (33)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIFrom EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIRating: 4 out of 5 stars4/5 (20)