You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- CTC 450 Review: Guide to Stabilization Pond ProcessesDocument12 pagesCTC 450 Review: Guide to Stabilization Pond ProcessesMansi Kakani BurhadeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Savitribai Phule Pune University UG Credit System RulesDocument11 pagesSavitribai Phule Pune University UG Credit System RulesMansi Kakani BurhadeNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Waste Water Treatment: A Guide to Primary, Secondary and Tertiary ProcessesDocument50 pagesWaste Water Treatment: A Guide to Primary, Secondary and Tertiary ProcessesMansi Kakani BurhadeNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Municipal Solid Wastes Rules 2000 SummaryDocument31 pagesMunicipal Solid Wastes Rules 2000 SummarySarish KumarNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- First Stage PresentationDocument23 pagesFirst Stage PresentationMansi Kakani BurhadeNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
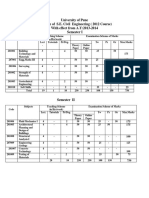
- T.E.civil 2012 Course SyllabusDocument26 pagesT.E.civil 2012 Course SyllabusHamidullah TotakhailNo ratings yet
- 853 Topper 21 116 1 4 7206 The Laws of Motion Up201507231545 1437646501 2479Document4 pages853 Topper 21 116 1 4 7206 The Laws of Motion Up201507231545 1437646501 2479Mansi Kakani BurhadeNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 852 Topper 21 116 1 4 7205 Moving Objects Up201507231544 1437646441 3319Document6 pages852 Topper 21 116 1 4 7205 Moving Objects Up201507231544 1437646441 3319Mansi Kakani BurhadeNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- T.E.civil 2012 Course SyllabusDocument26 pagesT.E.civil 2012 Course SyllabusHamidullah TotakhailNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 820 Topper 21 116 1 1 682 Cell The Unit of Life Up201507231524 1437645241 5531Document8 pages820 Topper 21 116 1 1 682 Cell The Unit of Life Up201507231524 1437645241 5531Mansi Kakani BurhadeNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- T.E.civil 2012 Course SyllabusDocument26 pagesT.E.civil 2012 Course SyllabusHamidullah TotakhailNo ratings yet
- 823 Topper 21 116 1 1 7220 Life Simple and Complex Up201507231533 1437645790 7855Document13 pages823 Topper 21 116 1 1 7220 Life Simple and Complex Up201507231533 1437645790 7855Mansi Kakani BurhadeNo ratings yet
- Civil Engineering 27-5-13Document39 pagesCivil Engineering 27-5-13Mansi Kakani BurhadeNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 851 Topper 21 116 1 4 7209 Energy The Driving Force Up201507231543 1437646395 3746Document5 pages851 Topper 21 116 1 4 7209 Energy The Driving Force Up201507231543 1437646395 3746Mansi Kakani BurhadeNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 200 Questions and Answers On Practical Civil Engineering Works 2008Document84 pages200 Questions and Answers On Practical Civil Engineering Works 2008ramdj100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Unit 01 Introduction To Fluid Statics and Flow Phenomena by TheDocument16 pagesUnit 01 Introduction To Fluid Statics and Flow Phenomena by TheMansi Kakani BurhadeNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- BUILDING MATERIALSDocument20 pagesBUILDING MATERIALSMansi Kakani BurhadeNo ratings yet
- Unit 03 Finite and Differential Control Volume Analysis by TheDocument10 pagesUnit 03 Finite and Differential Control Volume Analysis by TheMansi Kakani BurhadeNo ratings yet
- Unit 02 Fluid Dynamics and Kinematics by Stephanie The Saylor MechanicDocument11 pagesUnit 02 Fluid Dynamics and Kinematics by Stephanie The Saylor MechanicMansi Kakani BurhadeNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- MCQ 1 2 ExampleDocument1 pageMCQ 1 2 ExampleMusa Al-ShammaryNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Surveying Method Chosen Depends On:: - by The Purpose of The Survey E.G. Map MakingDocument27 pagesSurveying Method Chosen Depends On:: - by The Purpose of The Survey E.G. Map MakingAyaz AhmedNo ratings yet
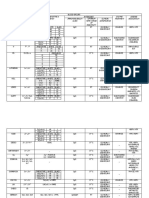
- TetracyclineDocument5 pagesTetracyclineapi-296073547No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Patch AdamsDocument14 pagesPatch AdamsNica Marie LumbaNo ratings yet
- Training Needs Assessment of Poultry Farmers in TeDocument4 pagesTraining Needs Assessment of Poultry Farmers in TeGia MNo ratings yet
- Vitamins and MineralsDocument25 pagesVitamins and MineralsFyan FiradyNo ratings yet
- 1 (7) Physiotherapy in Asthma Using The New Lotorp Method-IVA FAKHRIANI AMIRUDDINDocument4 pages1 (7) Physiotherapy in Asthma Using The New Lotorp Method-IVA FAKHRIANI AMIRUDDINIvha SmartNo ratings yet
- UNIT 10 (Urinary System)Document6 pagesUNIT 10 (Urinary System)Workinesh Kaynabo KambaloNo ratings yet
- RR 5417Document144 pagesRR 5417Handriyato SukmaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Chapter 2 RRLDocument3 pagesChapter 2 RRLMaribel Tan-Losloso NayadNo ratings yet
- Appliedand Economic ZoologyDocument3 pagesAppliedand Economic ZoologyNadeemNo ratings yet
- Raynaud 'S PhenomenonDocument3 pagesRaynaud 'S PhenomenonD Dzikrillah Danar SNo ratings yet
- Lect 10 - Acoelomate Bilateral AnimalsDocument42 pagesLect 10 - Acoelomate Bilateral AnimalsPriya DarshiniNo ratings yet
- TestDocument27 pagesTestHoàng ThọNo ratings yet
- Bloodvvimp 1Document13 pagesBloodvvimp 1ashokNo ratings yet
- Fish Physiology and Biochemistry MFSC SyllabusDocument19 pagesFish Physiology and Biochemistry MFSC SyllabusngonguyenminhtuanNo ratings yet
- Laporan Bulanan Rekapitulasi Hasil Deteksi Dini Hepatitis B Pada Ibu HamilDocument1 pageLaporan Bulanan Rekapitulasi Hasil Deteksi Dini Hepatitis B Pada Ibu HamilShanty SulamNo ratings yet
- Philippine Small Ruminants Industry Roadmap PDFDocument113 pagesPhilippine Small Ruminants Industry Roadmap PDFDA National Livestock ProgramNo ratings yet
- Practical Hematology Lab: RBC Morphology GuideDocument61 pagesPractical Hematology Lab: RBC Morphology GuideJefferson Soriano50% (2)
- @santoselizabeth 96Document2 pages@santoselizabeth 96ZabNo ratings yet
- Hedgehog Care SheetDocument9 pagesHedgehog Care Sheetapi-268266448No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 21 Tips to Keep Your Shit Together When DepressedDocument3 pages21 Tips to Keep Your Shit Together When DepressedPaul MayNo ratings yet
- URGENT - Casper, WY Contact: Cathy Corbin at 307-267-6524 or KahzieDocument3 pagesURGENT - Casper, WY Contact: Cathy Corbin at 307-267-6524 or KahzieAndy BovioNo ratings yet
- ELSI Core Manual April 2012Document90 pagesELSI Core Manual April 2012sacabonaNo ratings yet
- Developmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsDocument71 pagesDevelopmental Dysplasia of The Hip: Dr. Bassel El-Osta SPR Trauma & OrthopaedicsvadimmadanNo ratings yet
- Who TB - LtbiDocument38 pagesWho TB - LtbiC. S.No ratings yet
- Matt's Fault: The Foot Is A Phallic Symbol" Used To Describe Anyone Who Is Overly Concerned With Sex SymbolsDocument8 pagesMatt's Fault: The Foot Is A Phallic Symbol" Used To Describe Anyone Who Is Overly Concerned With Sex SymbolsbayuadNo ratings yet
- Female RTOG Normal Pelvis Atlas PDFDocument129 pagesFemale RTOG Normal Pelvis Atlas PDFsusdoctor100% (1)
- Blood Groups Assignment AaaDocument3 pagesBlood Groups Assignment AaaLoro JDNo ratings yet
- Underworld Lore Issue 02 PDFDocument56 pagesUnderworld Lore Issue 02 PDFFoxtrot Oscar100% (3)
- Be It Ordained by The Sangguniang Panlungsod of The City of San Carlos, Province of Negros Occidental in Regular Session Assembled ThatDocument7 pagesBe It Ordained by The Sangguniang Panlungsod of The City of San Carlos, Province of Negros Occidental in Regular Session Assembled ThatJayson CalbanNo ratings yet
- Assesing A Casualty Vital SignsDocument19 pagesAssesing A Casualty Vital SignsCiedelle Honey Lou DimaligNo ratings yet