You might also like
- Completo CF PDFDocument221 pagesCompleto CF PDFDoménica Córdova75% (4)
- Completo CF PDFDocument221 pagesCompleto CF PDFDoménica Córdova75% (4)
- Completo CF PDFDocument221 pagesCompleto CF PDFDoménica Córdova75% (4)
- Denver II Test Form PDFDocument2 pagesDenver II Test Form PDFFiorellaBeatriz100% (4)
- ABC checklist autism behaviorsDocument2 pagesABC checklist autism behaviorsAdriane Carqueijo100% (1)
- ABC checklist autism behaviorsDocument2 pagesABC checklist autism behaviorsAdriane Carqueijo100% (1)
- AQ Child Scoring KeyDocument3 pagesAQ Child Scoring Keydanielaica21100% (1)
- ASQ-3 English QuestionnaireDocument6 pagesASQ-3 English QuestionnairetaxidiaraNo ratings yet
- Ages and Stages 24 Months QuestionairreDocument8 pagesAges and Stages 24 Months QuestionairreandikaisnaeniNo ratings yet
- Mchat DOTorgDocument2 pagesMchat DOTorgtraviscNo ratings yet
- Month Questionnaire: Ages & Stages QuestionnairesDocument6 pagesMonth Questionnaire: Ages & Stages QuestionnairesDeff HaningNo ratings yet
- The Dyssemia Rating Scale (DRS) - School Screening GuideDocument8 pagesThe Dyssemia Rating Scale (DRS) - School Screening GuideHazardous7No ratings yet
- A Stress Test For ChildrenDocument2 pagesA Stress Test For ChildrenVasiloni Ioan PaulNo ratings yet
- Piccolo Sample ItemsDocument1 pagePiccolo Sample Itemsapi-432499175No ratings yet
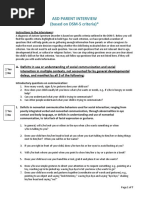
- ASD Questionnaire For ParentsDocument8 pagesASD Questionnaire For ParentsSuleman Malik100% (1)
- Microsoft Excel Shortcut Keys PDFDocument8 pagesMicrosoft Excel Shortcut Keys PDFrayNo ratings yet
- Paul Gilbert VIP LessonsDocument60 pagesPaul Gilbert VIP LessonsDavid Alejandro Mendez Licona83% (12)
- 3 Year Questionnaire PDFDocument8 pages3 Year Questionnaire PDFSurabhi Gupta ThakurNo ratings yet
- Month Questionnaire: Child's NameDocument7 pagesMonth Questionnaire: Child's NameKey KeyNo ratings yet
- Asq 3 54 M PDFDocument8 pagesAsq 3 54 M PDFnay nayNo ratings yet
- The Bayley Scales of InfantDocument10 pagesThe Bayley Scales of InfantJESUS MARTIN VILLA CARRASCONo ratings yet
- Asq For Parents PacketDocument4 pagesAsq For Parents Packetapi-422038067No ratings yet
- 4 Year Questionnaire PDFDocument8 pages4 Year Questionnaire PDFSurabhi Gupta ThakurNo ratings yet
- Asq 3 6 M PDFDocument7 pagesAsq 3 6 M PDFnay nayNo ratings yet
- Ages and Stages 9 Months QuestionairreDocument7 pagesAges and Stages 9 Months QuestionairreimuthandchaNo ratings yet
- Short Sensory ProfileDocument2 pagesShort Sensory ProfileFatima Zahra PatelNo ratings yet
- Ages and Stages 18 Months QuestionairreDocument7 pagesAges and Stages 18 Months QuestionairreKusuma RamadhaniNo ratings yet
- CARSDocument18 pagesCARSzarish.shireenNo ratings yet
- Modified Checklist For Autism in Toddlers, Revised (M-CHAT-R)Document3 pagesModified Checklist For Autism in Toddlers, Revised (M-CHAT-R)Siswand BIn Mohd AliNo ratings yet
- BRIEF2 Fact SheetDocument2 pagesBRIEF2 Fact Sheethamzabtoush02No ratings yet
- ACT - Child and Adolescent Intake Questionnaire PDFDocument16 pagesACT - Child and Adolescent Intake Questionnaire PDFPatty CrawfordNo ratings yet
- M Chat R - F PDFDocument25 pagesM Chat R - F PDFIuliana PanaitNo ratings yet
- Abas IIDocument11 pagesAbas IIMargarita Rosales IbáñezNo ratings yet
- Childhood Developmental History FormDocument5 pagesChildhood Developmental History FormMariya KhanNo ratings yet
- Month Questionnaire: Ages & Stages QuestionnairesDocument7 pagesMonth Questionnaire: Ages & Stages QuestionnairesamaliakhoirunnisaNo ratings yet
- Gross Motor 1 2: ST NDDocument3 pagesGross Motor 1 2: ST NDIloveshairavenice BundangNo ratings yet
- Asq 5yrsDocument9 pagesAsq 5yrsapi-349363475No ratings yet
- GmfmscoresheetDocument6 pagesGmfmscoresheetapi-260049180No ratings yet
- What is an Articulation ProblemDocument3 pagesWhat is an Articulation ProblemErrorry JecksonNo ratings yet
- Autism ChecklistDocument3 pagesAutism ChecklistAmes0% (1)
- The Wessex Head Injury MatrixDocument11 pagesThe Wessex Head Injury MatrixLiz GonzálezNo ratings yet
- M Chat ScoringDocument2 pagesM Chat ScoringAmir ShenoudaNo ratings yet
- Subjective Peripheral Neuropathy Screen QuestionnaireDocument1 pageSubjective Peripheral Neuropathy Screen QuestionnaireresearchNo ratings yet
- S3 CARS 2 SampleWriteUp 1Document1 pageS3 CARS 2 SampleWriteUp 1Janet FernandezNo ratings yet
- Autism Spectrum Disorder Final HandoutDocument2 pagesAutism Spectrum Disorder Final Handoutapi-264629576No ratings yet
- Diagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Document17 pagesDiagnosing Autism-Analyses of Data From The Autism Diagnostic Interview-CASO 3Betania MendozaNo ratings yet
- Reaching Out Autism Related MaterialsDocument14 pagesReaching Out Autism Related MaterialsArunasis AdhikariNo ratings yet
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocument2 pagesThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- ADHD Scoring InstructionsDocument1 pageADHD Scoring Instructionsnaseeruddin1No ratings yet
- Spence Children's Anxiety ScaleDocument3 pagesSpence Children's Anxiety ScaleAnnie AlvaradoNo ratings yet
- Parent Intake Questionnaire PDFDocument7 pagesParent Intake Questionnaire PDFMonica TrabancoNo ratings yet
- About Case Studies of ADHD in Childre1Document6 pagesAbout Case Studies of ADHD in Childre1PearlCladelLapidezNo ratings yet
- Hanen Tips EnglishDocument6 pagesHanen Tips EnglishGökçe Gökçümen KocaNo ratings yet
- Asd-Parent-Interview Formatted 2012 0325 PDFDocument7 pagesAsd-Parent-Interview Formatted 2012 0325 PDFVivek SagarNo ratings yet
- Childhood Autism Rating ScaleDocument2 pagesChildhood Autism Rating ScaleAsmaa ElarabyNo ratings yet
- ThePortageProject (GROUP)Document20 pagesThePortageProject (GROUP)saharNo ratings yet
- 9 Month Asq3 2Document10 pages9 Month Asq3 2api-377093974No ratings yet
- Road Advisors: Massachusetts Driver's LicenseDocument35 pagesRoad Advisors: Massachusetts Driver's LicenseDavid Gonzalez100% (1)
- Asq 3 8 M PDFDocument7 pagesAsq 3 8 M PDFAnsh AncaNo ratings yet
- Developmental Delay & Autism Spectrum Disorder Screening ToolsDocument5 pagesDevelopmental Delay & Autism Spectrum Disorder Screening ToolsTanFransisca DianNo ratings yet
- Autism Spectrum Screening QuestionnaireDocument2 pagesAutism Spectrum Screening QuestionnaireLana AkoNo ratings yet
- ASD Parent Interview Early ChildhoodDocument4 pagesASD Parent Interview Early ChildhoodritaNo ratings yet
- AUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONDocument5 pagesAUTISM IN CHILDREN: SIGNS, ASSESSMENT AND INTERVENTIONvai2No ratings yet
- CSBS DP Infant-Toddler Checklist: Emotion and Eye GazeDocument3 pagesCSBS DP Infant-Toddler Checklist: Emotion and Eye GazeDesislava PeevaNo ratings yet
- Neurological Assessment in the First Two Years of LifeFrom EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniNo ratings yet
- Connie’s Gifts- Interactive Books and Collectibles. Got Parenting Challenges? Book 1From EverandConnie’s Gifts- Interactive Books and Collectibles. Got Parenting Challenges? Book 1No ratings yet
- Brazilian Adaptation of The Addenbrooke's Cognitive Examination-Revised (ACE-R)Document5 pagesBrazilian Adaptation of The Addenbrooke's Cognitive Examination-Revised (ACE-R)Adriane CarqueijoNo ratings yet
- SintaxeDocument1 pageSintaxeTerceira Idade - O Envelhecimento HumanoNo ratings yet
- ASQ-3 12 Mo Set B PDFDocument7 pagesASQ-3 12 Mo Set B PDFAdriane CarqueijoNo ratings yet
- Cdi ManualDocument50 pagesCdi ManualJosue CuzcanoNo ratings yet
- Memoria VisualDocument238 pagesMemoria VisualHector Sancca Tito83% (6)
- Visual Closure Cierre VisualDocument221 pagesVisual Closure Cierre VisualBlanca Espinal100% (3)
- Tarjetas Wisconsin PDFDocument17 pagesTarjetas Wisconsin PDFAdriane CarqueijoNo ratings yet
- Denver II OverviewDocument33 pagesDenver II OverviewAgitha Melita PutriNo ratings yet
- Actividades Entrenamiento Habilidades Viso-PerceptivasDocument236 pagesActividades Entrenamiento Habilidades Viso-Perceptivasestherpdv100% (3)
- Latihan Soal On Line Kls 4Document4 pagesLatihan Soal On Line Kls 4Sumiyah CummyNo ratings yet
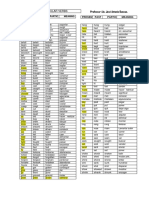
- Irregular Verbs Nueva Lista DuncanDocument2 pagesIrregular Verbs Nueva Lista DuncanAndrey Vargas MoralesNo ratings yet
- Linguistics Midterm TopicsDocument5 pagesLinguistics Midterm TopicsMadeline LeeahNo ratings yet
- CSS Grid Layout Guide - Everything You Need to KnowDocument11 pagesCSS Grid Layout Guide - Everything You Need to KnowSouvik Babai Roy100% (1)
- Cambridge IGCSE™: Computer Science 0478/22 February/March 2022Document11 pagesCambridge IGCSE™: Computer Science 0478/22 February/March 2022TrynosNo ratings yet
- Anatomy Paper ScopusDocument10 pagesAnatomy Paper ScopusNs. Iman Nurjaman, M.KepNo ratings yet
- Aristotle Study of TragedyDocument14 pagesAristotle Study of TragedyMohan VankudothNo ratings yet
- Irismodule AutismDocument4 pagesIrismodule Autismapi-585078296No ratings yet
- MLII Modbus Mapping Manual FV 4-33-05Document118 pagesMLII Modbus Mapping Manual FV 4-33-05Sergio SosaNo ratings yet
- Programming GuideDocument119 pagesProgramming GuideMarcosNo ratings yet
- Lesson 13Document7 pagesLesson 13api-382473176No ratings yet
- (ThichTiengAnh - Com) Tong Hop de Thi Tuyen Sinh Vao Lop 10 Mon Tieng Anh Cac TinhDocument25 pages(ThichTiengAnh - Com) Tong Hop de Thi Tuyen Sinh Vao Lop 10 Mon Tieng Anh Cac TinhQuynh NguyenNo ratings yet
- English Diff Instruction OFFICIAL SPN21 SOW YR8Document15 pagesEnglish Diff Instruction OFFICIAL SPN21 SOW YR8Yenny TigaNo ratings yet
- Infinitivi, Gerund, ParticipiDocument6 pagesInfinitivi, Gerund, ParticipiMartinaNo ratings yet
- Kids 2: INSTITUTO CAMBRIDGE de Cultura Inglesa - EXÁMENES 2019Document3 pagesKids 2: INSTITUTO CAMBRIDGE de Cultura Inglesa - EXÁMENES 2019Evaluna MoidalNo ratings yet
- Opimod 8200Document84 pagesOpimod 8200UTC_ITSNo ratings yet
- Expert Project Manager with 12+ Years ExperienceDocument3 pagesExpert Project Manager with 12+ Years ExperienceAshish SharmaNo ratings yet
- Our PoemDocument6 pagesOur Poemapi-213540529No ratings yet
- Excel Grade 5 LessPlans Mod 3Document24 pagesExcel Grade 5 LessPlans Mod 3Narine HovhannisyanNo ratings yet
- How To Ace Your IELTS Writing TestDocument19 pagesHow To Ace Your IELTS Writing TestAnindia AuliaNo ratings yet
- 38 Most Common Fiction Writing Mistakes (And How To Avoid Them)Document43 pages38 Most Common Fiction Writing Mistakes (And How To Avoid Them)1265uNo ratings yet
- Computer Networks Question BankDocument3 pagesComputer Networks Question BankNitin BirariNo ratings yet
- Max Duncker - The History of Antiquity - Volume 3Document472 pagesMax Duncker - The History of Antiquity - Volume 3Lucas MateusNo ratings yet
- Sams Asp Dotnet Evolution Isbn0672326477Document374 pagesSams Asp Dotnet Evolution Isbn0672326477paulsameeNo ratings yet
- Wangeela YohaannisVOL04 Oromo-1Document446 pagesWangeela YohaannisVOL04 Oromo-1Chala GetaNo ratings yet
- Result Gazette HSSC I A 218 PDFDocument819 pagesResult Gazette HSSC I A 218 PDFASIM RIAZNo ratings yet
- Jurnal 3 2019Document8 pagesJurnal 3 2019Nur AfiyatNo ratings yet
- "Sure, I Did The Right Thing": A System For Sarcasm Detection in SpeechDocument5 pages"Sure, I Did The Right Thing": A System For Sarcasm Detection in SpeechRoberto RodNo ratings yet