You might also like
- Month Questionnaire: Ages & Stages QuestionnairesDocument6 pagesMonth Questionnaire: Ages & Stages QuestionnairesDeff HaningNo ratings yet
- A Blind Child's Pathway to Learning: Developing Cognition Without SightFrom EverandA Blind Child's Pathway to Learning: Developing Cognition Without SightNo ratings yet
- Asq 3 6 M PDFDocument7 pagesAsq 3 6 M PDFnay nayNo ratings yet
- Ages and Stages 18 Months QuestionairreDocument7 pagesAges and Stages 18 Months QuestionairreKusuma RamadhaniNo ratings yet
- ASQ-3 English QuestionnaireDocument6 pagesASQ-3 English QuestionnairetaxidiaraNo ratings yet
- Asq 3 42 MDocument8 pagesAsq 3 42 MMohammed AlsuwaidiNo ratings yet
- 3 Year Questionnaire PDFDocument8 pages3 Year Questionnaire PDFSurabhi Gupta ThakurNo ratings yet
- Asq 3 8 M PDFDocument7 pagesAsq 3 8 M PDFAnsh AncaNo ratings yet
- Asq 5yrsDocument9 pagesAsq 5yrsapi-349363475No ratings yet
- Ages and Stages 24 Months QuestionairreDocument8 pagesAges and Stages 24 Months QuestionairreandikaisnaeniNo ratings yet
- Ages and Stages 9 Months QuestionairreDocument7 pagesAges and Stages 9 Months QuestionairreimuthandchaNo ratings yet
- 4 Year Questionnaire PDFDocument8 pages4 Year Questionnaire PDFSurabhi Gupta ThakurNo ratings yet
- Asq 3 54 M PDFDocument8 pagesAsq 3 54 M PDFnay nayNo ratings yet
- SCREENING - DEVELOPMENTAL DELAY & AUTISM - CCBS DP Infant-Toddler ChecklistDocument9 pagesSCREENING - DEVELOPMENTAL DELAY & AUTISM - CCBS DP Infant-Toddler ChecklistMihaela Grigoroiu100% (1)
- PEDS and ASQ Developmental Screening TestsDocument10 pagesPEDS and ASQ Developmental Screening TestsSuryani Malik100% (1)
- Asq For Parents PacketDocument4 pagesAsq For Parents Packetapi-422038067No ratings yet
- Screening Tool ManualDocument17 pagesScreening Tool ManualSupriadi HardiantoNo ratings yet
- Modified Checklist For Autism in Toddlers, Revised (M-CHAT-R)Document3 pagesModified Checklist For Autism in Toddlers, Revised (M-CHAT-R)Siswand BIn Mohd AliNo ratings yet
- Testing and Beyond - Strategies and Tools For Evaluating and Assessing Infants and ToddlersDocument25 pagesTesting and Beyond - Strategies and Tools For Evaluating and Assessing Infants and ToddlersMargareta Salsah BeeNo ratings yet
- Construção Da DemocraciaDocument44 pagesConstrução Da DemocraciaLina LopesNo ratings yet
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocument2 pagesThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- Early Stimulation and Development ActivitiesDocument63 pagesEarly Stimulation and Development ActivitiesRucsandra AvirvareiNo ratings yet
- Bayley ScalesDocument7 pagesBayley Scalesmrabhilekh100% (1)
- Sensory Regulation ConferenceDocument19 pagesSensory Regulation ConferenceSebastian Pinto ReyesNo ratings yet
- Sample: Sensory Processing Measure-PreschoolDocument1 pageSample: Sensory Processing Measure-PreschoolQORI KARUNIA WANTINo ratings yet
- GmfmscoresheetDocument6 pagesGmfmscoresheetapi-260049180No ratings yet
- DSC BookDocument52 pagesDSC BookPriti Khemka60% (5)
- Developmental Milestones Motor Development - Peds Rev 2010Document13 pagesDevelopmental Milestones Motor Development - Peds Rev 2010Carolina SanchezNo ratings yet
- Month Questionnaire: Ages & Stages QuestionnairesDocument7 pagesMonth Questionnaire: Ages & Stages QuestionnairesAdriane CarqueijoNo ratings yet
- Hanen Tips EnglishDocument6 pagesHanen Tips EnglishGökçe Gökçümen KocaNo ratings yet
- The Bayley Scales of InfantDocument10 pagesThe Bayley Scales of InfantJESUS MARTIN VILLA CARRASCONo ratings yet
- Short Sensory ProfileDocument11 pagesShort Sensory ProfileNurul Izzah Wahidul Azam100% (1)
- Sensory Profile 2 (SP2) : Age Range: Time To AdministerDocument3 pagesSensory Profile 2 (SP2) : Age Range: Time To Administer宗轶烜No ratings yet
- Movement ABC 2 Frequently Asked QuestionsDocument8 pagesMovement ABC 2 Frequently Asked QuestionsCat Graverobber Iskariot0% (1)
- Occupational Therapy Ia Sample ReportsDocument11 pagesOccupational Therapy Ia Sample Reportssneha duttaNo ratings yet
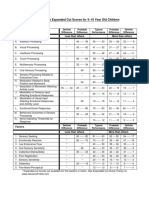
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 pageSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNo ratings yet
- Sensory History QuestionnaireDocument6 pagesSensory History Questionnaireİpek OMUR100% (1)
- Chapter 8Document30 pagesChapter 8Karla CarazoNo ratings yet
- Developmental ChecklistDocument15 pagesDevelopmental Checklistapi-339989449No ratings yet
- Pediatric Wheelchair Toolkit FINALDocument6 pagesPediatric Wheelchair Toolkit FINALIndiana Family to FamilyNo ratings yet
- 6 (SPM™) Sensory Processing Measure™ - WPSDocument1 page6 (SPM™) Sensory Processing Measure™ - WPSVINEET GAIROLANo ratings yet
- Feeding Problems in Children with ASD ReviewDocument15 pagesFeeding Problems in Children with ASD ReviewNina Salinas100% (1)
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoNo ratings yet
- Mchat DOTorgDocument2 pagesMchat DOTorgtraviscNo ratings yet
- Using The Developmental Assessment of Young Children (DAYC) : Jefferson Digital CommonsDocument38 pagesUsing The Developmental Assessment of Young Children (DAYC) : Jefferson Digital Commonsvivien100% (1)
- DAYC Assessment GuideDocument38 pagesDAYC Assessment Guidemaya damayantiNo ratings yet
- BriganceDocument1 pageBriganceamf780% (1)
- Sensory Integration and Praxis Patterns in Children With AutismDocument9 pagesSensory Integration and Praxis Patterns in Children With AutismadriricaldeNo ratings yet
- Peabody y Movent ABCDocument11 pagesPeabody y Movent ABCIngrid BarkoNo ratings yet
- SPM IntroduccionDocument20 pagesSPM IntroduccionConstanzaNo ratings yet
- Feeding GuideDocument6 pagesFeeding GuideDorneanu Alexandru100% (1)
- 15 Selected Assess Tools For ASDDocument15 pages15 Selected Assess Tools For ASDSrinivas Achary100% (1)
- CASBY Developmental Assessment of Play PDFDocument10 pagesCASBY Developmental Assessment of Play PDFElizabeth SoutulloNo ratings yet
- Assessment Review - Cars2Document11 pagesAssessment Review - Cars2api-3151104170% (1)
- Selected Developmental Screening Tools A Resource For Early EducatorsDocument60 pagesSelected Developmental Screening Tools A Resource For Early EducatorsEva Sala RenauNo ratings yet
- PEDS Score FormDocument4 pagesPEDS Score FormNor SyamimiNo ratings yet
- Sample Report: Dyslexia Early Screening Test - Second Edition (DEST-2)Document5 pagesSample Report: Dyslexia Early Screening Test - Second Edition (DEST-2)Mudassar HussainNo ratings yet
- INFANIBDocument8 pagesINFANIBandrea sierraNo ratings yet
- BDI-2 Assessment ToolDocument42 pagesBDI-2 Assessment ToolJesus Fernandez100% (1)
- Asq 3 20 MDocument7 pagesAsq 3 20 MfreNo ratings yet
- Ages and Stages 24 Months QuestionairreDocument8 pagesAges and Stages 24 Months QuestionairreandikaisnaeniNo ratings yet
- Nilai Batch 6Document24 pagesNilai Batch 6amaliakhoirunnisaNo ratings yet
- The role of insects in food security, livelihoods and the environmentDocument4 pagesThe role of insects in food security, livelihoods and the environmentamaliakhoirunnisaNo ratings yet
- OtienoDocument321 pagesOtienoamaliakhoirunnisaNo ratings yet
- Good Night Sleep Tight PDFDocument382 pagesGood Night Sleep Tight PDFDanny BoysieNo ratings yet
- Final Paper Media LitDocument61 pagesFinal Paper Media Litapi-529621196No ratings yet
- Reflection PaperDocument2 pagesReflection Paperapi-544776411No ratings yet
- IntoeingDocument2 pagesIntoeingJackyNo ratings yet
- Growth Monitoring ManualDocument202 pagesGrowth Monitoring ManualHarshith TammuNo ratings yet
- AZECA Child Care Infographic FINALDocument2 pagesAZECA Child Care Infographic FINALcronkitenewsNo ratings yet
- Ngo: Udayan Care: Volunteer Work Report Course: Social Awareness Program (SAP)Document10 pagesNgo: Udayan Care: Volunteer Work Report Course: Social Awareness Program (SAP)SHUBHAM BHASKAR BADHE MBA 2021-23 DelhiNo ratings yet
- Kids in The Atrium Comparing Architectural Intentions and Childrens Experiences in A Pediatric Hospital LobbyDocument10 pagesKids in The Atrium Comparing Architectural Intentions and Childrens Experiences in A Pediatric Hospital LobbySergio CancinoNo ratings yet
- Victorian Era ResearchDocument8 pagesVictorian Era Researchmiftha syahriaNo ratings yet
- Sociologist argues concerns over children's entertainment not newDocument3 pagesSociologist argues concerns over children's entertainment not newTiphanie KangNo ratings yet
- American Academy of Pediatrics (WI Chapter) Opposition To AB163 Statute To Require Anti-Choking Devices in Schools (7/20/23)Document2 pagesAmerican Academy of Pediatrics (WI Chapter) Opposition To AB163 Statute To Require Anti-Choking Devices in Schools (7/20/23)Auntie QuackeryNo ratings yet
- Classroom AccommodationsDocument13 pagesClassroom AccommodationsTiffany InocenteNo ratings yet
- Rojina Basnet Roll No: 3 MPHN (1 Batch)Document24 pagesRojina Basnet Roll No: 3 MPHN (1 Batch)rojinaNo ratings yet
- Local Baby Diaper Makers Seek Larger ShareDocument6 pagesLocal Baby Diaper Makers Seek Larger ShareMehedi HasanNo ratings yet
- Erikson's Psychosocial DevelopmentDocument38 pagesErikson's Psychosocial DevelopmentAmeil OrindayNo ratings yet
- Facts For Life Brochure en 010810Document4 pagesFacts For Life Brochure en 010810NO NAMENo ratings yet
- MSWD Operation of Day Care Services ProgramDocument2 pagesMSWD Operation of Day Care Services ProgramMonteza Dela Serna100% (1)
- Blood Relation Quiz 4Document10 pagesBlood Relation Quiz 4BhimNo ratings yet
- Life ContinuesDocument70 pagesLife ContinuesEmma ForgácsNo ratings yet
- Breastfeeding: Proper Positioning and Latch-On SkillsDocument4 pagesBreastfeeding: Proper Positioning and Latch-On SkillsEdmr SlzarNo ratings yet
- Kangaroo Care Method Raises Body Temperature in LBW BabiesDocument4 pagesKangaroo Care Method Raises Body Temperature in LBW BabiesSisca AngrianingsihNo ratings yet
- Choking: What To Do If A Child Is Choking?Document3 pagesChoking: What To Do If A Child Is Choking?Jamieson TobeyNo ratings yet
- Nurse RoleDocument1 pageNurse RolechoobiNo ratings yet
- Development Assessment: Dr. Hodan AhmedDocument30 pagesDevelopment Assessment: Dr. Hodan Ahmedmukhtar abddiNo ratings yet
- Jonas' Journey as the New Receiver Begins"TITLE"The Apprehensive Jonas is Selected as the Next Receiver" TITLE"Jonas Learns of His Important Role and Training as ReceiverDocument11 pagesJonas' Journey as the New Receiver Begins"TITLE"The Apprehensive Jonas is Selected as the Next Receiver" TITLE"Jonas Learns of His Important Role and Training as ReceiverVenus Yeung100% (1)
- ADVIENTO, MIA CZARINA C. - Newborn ReflexDocument2 pagesADVIENTO, MIA CZARINA C. - Newborn ReflexMia Czarina AdvientoNo ratings yet
- March To 14 April 2020 - Login Access To Be Advised Later)Document1 pageMarch To 14 April 2020 - Login Access To Be Advised Later)aqem222No ratings yet
- Drugs ActivityDocument1 pageDrugs ActivityISTJ hohohoNo ratings yet
- Effects of Cyberbullying on Teens' Mental HealthDocument4 pagesEffects of Cyberbullying on Teens' Mental HealthRommel SerantesNo ratings yet
- CHN Family Developmental StagesDocument12 pagesCHN Family Developmental StagesRyll JohnsonNo ratings yet