You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Admission Criteria Dengue FeverDocument23 pagesAdmission Criteria Dengue FeverMuhammad Luthfi TaufikNo ratings yet
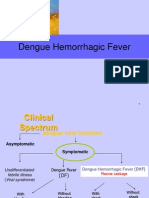
- Dengue Hemorrhagic FeverDocument27 pagesDengue Hemorrhagic FeverTristiana DewiNo ratings yet
- DENGUE Clinician GuideDocument8 pagesDENGUE Clinician GuideLuis Alfredo LaraNo ratings yet
- Dengue TreamentDocument2 pagesDengue TreamentKevin ChanNo ratings yet
- WHO Dengue Classification and Case Management-FlyerDocument2 pagesWHO Dengue Classification and Case Management-FlyerKathleen DyNo ratings yet
- Lapjag Bangsal IPD 22 OKTOBER DHFDocument57 pagesLapjag Bangsal IPD 22 OKTOBER DHFLeony Nerry SabatiniNo ratings yet
- CholeraDocument5 pagesCholerabishnu011978No ratings yet
- Dengue FinalDocument44 pagesDengue FinalAniket MuleNo ratings yet
- Hema Case 2Document55 pagesHema Case 2jlcocm-2022-00028No ratings yet
- IV Therapy SlidesDocument8 pagesIV Therapy SlidesRegean MercadoNo ratings yet
- Dengue Report (For Checking)Document34 pagesDengue Report (For Checking)Mark ReyesNo ratings yet
- Dengue: Denggoy, Dengvaxia, Dengue Ba Sya?Document55 pagesDengue: Denggoy, Dengvaxia, Dengue Ba Sya?KatNo ratings yet
- Fever: DengueDocument95 pagesFever: DengueAnonymous RNMJmeu8tNo ratings yet
- 79 - Dengue and Dengue Shock SyndromeDocument5 pages79 - Dengue and Dengue Shock SyndromeCeejhay Lee0% (1)
- Pedia ReviewerDocument27 pagesPedia ReviewerEvangeline GoNo ratings yet
- Management Severe DengueDocument18 pagesManagement Severe DengueMuhammad Fhandeka IsrarNo ratings yet
- Dengue - IV Fluid PrinciplesDocument25 pagesDengue - IV Fluid PrinciplesArjuna BuduhNo ratings yet
- Dengu Syndrome & Its Managment - Prof. Kaka1Document39 pagesDengu Syndrome & Its Managment - Prof. Kaka1Aditi SahaNo ratings yet
- Chole CystitisDocument61 pagesChole CystitisPlain GerlNo ratings yet
- Dengue FeverDocument9 pagesDengue FeverAmy TabassumNo ratings yet
- Sample Case Presentation - Occult BacteremiaDocument51 pagesSample Case Presentation - Occult BacteremiaPrecious Gutierrez BagazinNo ratings yet
- Dengue Update: Gan Kai XinDocument40 pagesDengue Update: Gan Kai XinKai XinNo ratings yet
- Pakistan Dengue Management 14.9.11Document103 pagesPakistan Dengue Management 14.9.11Tehreem JavedNo ratings yet
- Lascano, Joanne Alyssa - RheumatologyDocument13 pagesLascano, Joanne Alyssa - RheumatologyJoanne Alyssa Hernandez LascanoNo ratings yet
- Blood Components and Blood TransfusionDocument38 pagesBlood Components and Blood TransfusionjosephNo ratings yet
- Dengue Fever - Ang Ban HongDocument46 pagesDengue Fever - Ang Ban HongSharimanfadhly YahayaNo ratings yet
- Dengue: West Visayas State University-Medical Center Department of PediatricsDocument89 pagesDengue: West Visayas State University-Medical Center Department of PediatricsVanessa YunqueNo ratings yet
- Fluids&LytesDocument33 pagesFluids&LytesMateen ShukriNo ratings yet
- Nephrotic SyndromeDocument20 pagesNephrotic Syndromeami5687No ratings yet
- Fluid Management in Dengue Hemorrhagic FeverDocument38 pagesFluid Management in Dengue Hemorrhagic FeverMarvin OcampoNo ratings yet
- Dengue Who ProtocolDocument48 pagesDengue Who ProtocolariefzandoNo ratings yet
- Dengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease SpecialistDocument48 pagesDengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease SpecialistariefzandoNo ratings yet
- Exchange TransfusionDocument9 pagesExchange TransfusiondewpraNo ratings yet
- Dengue FinalDocument24 pagesDengue FinalManju ManjunathNo ratings yet
- IM Case ReportDocument5 pagesIM Case ReportGurungSurajNo ratings yet
- Dengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease SpecialistDocument48 pagesDengue: Who Guidelines For Diagnosis and Treatment: Jimmy Mendigo, MD Infectious Disease Specialistkristianus yantoNo ratings yet
- Reaksi TransfusiDocument5 pagesReaksi TransfusiInatrinNo ratings yet
- Pengkajian Primer Sekunder 2018Document20 pagesPengkajian Primer Sekunder 2018dewirinjanimNo ratings yet
- Transfusion Process For NursesDocument31 pagesTransfusion Process For NursesShoheb ShaikhNo ratings yet
- Recommendations For Sepsis Management in Limited SourcesDocument25 pagesRecommendations For Sepsis Management in Limited SourcesFatahillah NazarNo ratings yet
- Management Dengue HXDocument6 pagesManagement Dengue HXMalshika JayatissaNo ratings yet
- Dengue PPT YaarDocument21 pagesDengue PPT YaarY ShouryaNo ratings yet
- Iat Sepsis v7 3Document1 pageIat Sepsis v7 3api-296123515No ratings yet
- 11.pearls in Paediatric Haematology - PART 2 SUMMARY - 082022Document42 pages11.pearls in Paediatric Haematology - PART 2 SUMMARY - 082022Cedric KyekyeNo ratings yet
- DISEASES CASE MANAGEMENT PROTOCOL Final Draft DTD August 2014-VaidDocument34 pagesDISEASES CASE MANAGEMENT PROTOCOL Final Draft DTD August 2014-VaidferasNo ratings yet
- Paediatric Septic Shock: Corrine BalitDocument37 pagesPaediatric Septic Shock: Corrine BalitJauhari DesloNo ratings yet
- Shock in Children TutorialDocument37 pagesShock in Children TutorialSsenyonga DominicNo ratings yet
- Abnormal Midwifery1 1Document352 pagesAbnormal Midwifery1 1Mary AndrewNo ratings yet
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDocument352 pagesAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNo ratings yet
- Emergency Management of BurnDocument47 pagesEmergency Management of BurnBudhi Nath Adhikari100% (1)
- Dengue: Pgi Salem, Freya AngelaDocument70 pagesDengue: Pgi Salem, Freya AngelaFreya Angela Laurente SalemNo ratings yet
- Blood and Blood Components-LectureDocument13 pagesBlood and Blood Components-LectureMelissa GinesNo ratings yet
- Dengue Hemorrhagic Fever IIIDocument28 pagesDengue Hemorrhagic Fever IIIJehrisse L. Soriano-OcampoNo ratings yet
- Dengue Spectrum FinalDocument43 pagesDengue Spectrum Finalshyam kumar MishraNo ratings yet
- A Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to Blood in Stools, Related Diseases and Use in Disease DiagnosisRating: 3 out of 5 stars3/5 (1)
- Mathematical Model CNSDocument24 pagesMathematical Model CNSjmbobitNo ratings yet
- Intergroup Phase III RCT On Unresectable Head and Neck CancersDocument7 pagesIntergroup Phase III RCT On Unresectable Head and Neck CancersjmbobitNo ratings yet
- NCD in Poor CountriesDocument6 pagesNCD in Poor CountriesjmbobitNo ratings yet
- Quick Reference Citation FormatDocument8 pagesQuick Reference Citation FormatjmbobitNo ratings yet