You might also like
- Blood Transfusion Reactions: Life Saving Yet Life ThreateningDocument52 pagesBlood Transfusion Reactions: Life Saving Yet Life Threateninganam farzand100% (2)
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsarifgteguhNo ratings yet
- Blood Transfusion - Megha SoniDocument29 pagesBlood Transfusion - Megha SoniMegha VadanereNo ratings yet
- Blood Components and Blood TransfusionDocument38 pagesBlood Components and Blood TransfusionjosephNo ratings yet
- Blood Component Therapy F17Document33 pagesBlood Component Therapy F17Crystal LynaeNo ratings yet
- Blood Transfusion and Conservation: Dr. T.C. KriplaniDocument45 pagesBlood Transfusion and Conservation: Dr. T.C. KriplaniParvathy R NairNo ratings yet
- Advanced Clinical Pharmacology Jan 2009Document51 pagesAdvanced Clinical Pharmacology Jan 2009kylietanglsNo ratings yet
- Adverse Effects: Blood TransfusionDocument43 pagesAdverse Effects: Blood TransfusionDumindu PereraNo ratings yet
- Blood TransfusionDocument41 pagesBlood TransfusionajNo ratings yet
- Transfusion Reaction - DRGSPDocument42 pagesTransfusion Reaction - DRGSPGaurav PawarNo ratings yet
- null7Document21 pagesnull7Muneeb Ur RehmanNo ratings yet
- Hema Case 2Document55 pagesHema Case 2jlcocm-2022-00028No ratings yet
- Surgery of Kidney Ureter and VaricoseDocument55 pagesSurgery of Kidney Ureter and VaricoseSaurabh SharmaNo ratings yet
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsAulia RahmanNo ratings yet
- Aedes aegypti Mosquito and Dengue VirusDocument34 pagesAedes aegypti Mosquito and Dengue VirusMark ReyesNo ratings yet
- Adverse Effects of Plasma TherapyDocument80 pagesAdverse Effects of Plasma TherapyShaiji ShahidNo ratings yet
- Rational Use of Safe BloodDocument22 pagesRational Use of Safe Bloodkamnasharma0907No ratings yet
- Blood TransfusionDocument41 pagesBlood TransfusionajNo ratings yet
- Transfusion Medicine OverviewDocument40 pagesTransfusion Medicine OverviewmonichaNo ratings yet
- BT New TemplateDocument65 pagesBT New TemplateNikky SilvestreNo ratings yet
- Blood & Blood ProductsDocument29 pagesBlood & Blood Productsneelam aliNo ratings yet
- Blood TransfusionDocument55 pagesBlood TransfusionEsther Ellise AbundoNo ratings yet
- BLOOD TRANSFUSION GUIDEDocument75 pagesBLOOD TRANSFUSION GUIDEKamal SaudNo ratings yet
- Transfusion Medicine ProtocolDocument9 pagesTransfusion Medicine ProtocolmedvettheoryNo ratings yet
- Blood Transfusion and Blood ProductsDocument26 pagesBlood Transfusion and Blood ProductsamvyellicamaricorcoNo ratings yet
- Blood Transfusion Blood Grouping and Cross MatchingDocument46 pagesBlood Transfusion Blood Grouping and Cross MatchingHa LeemNo ratings yet
- Transfusion Medicine by Dr. Sharad JohriDocument54 pagesTransfusion Medicine by Dr. Sharad JohriShashwat JohriNo ratings yet
- Adverse Blood Reaction and HDNDocument34 pagesAdverse Blood Reaction and HDNAdeniran CharlesNo ratings yet
- Blood Transfusion: Teoman SOYSAL Prof. MDDocument38 pagesBlood Transfusion: Teoman SOYSAL Prof. MDirdinamarchsyaNo ratings yet
- Dengue Fever - Ang Ban HongDocument46 pagesDengue Fever - Ang Ban HongSharimanfadhly YahayaNo ratings yet
- AHTR Acute Hemolytic Transfusion Reaction Symptoms Causes ManagementDocument5 pagesAHTR Acute Hemolytic Transfusion Reaction Symptoms Causes ManagementInatrinNo ratings yet
- Dengue: Denggoy, Dengvaxia, Dengue Ba Sya?Document55 pagesDengue: Denggoy, Dengvaxia, Dengue Ba Sya?KatNo ratings yet
- Division of Blood Transfusion Services: Ministry of Health and Family WelfareDocument46 pagesDivision of Blood Transfusion Services: Ministry of Health and Family WelfareKirandragonNo ratings yet
- Blood Transfusion Complications & Management (40Document30 pagesBlood Transfusion Complications & Management (40kushalNo ratings yet
- Transfusion Therapy (4!10!2016)Document32 pagesTransfusion Therapy (4!10!2016)vishnuNo ratings yet
- CPG DENGUE: A GUIDE TO DIAGNOSIS AND TREATMENTDocument35 pagesCPG DENGUE: A GUIDE TO DIAGNOSIS AND TREATMENTSharimanfadhly YahayaNo ratings yet
- Surgery Slide 6 - Blood TransfusionsDocument54 pagesSurgery Slide 6 - Blood TransfusionsEman NazzalNo ratings yet
- Capstone Project SlidesDocument24 pagesCapstone Project Slidesapi-545362109No ratings yet
- CLINICAL ASPECTS OF BLOOD TRANSFUSIONDocument37 pagesCLINICAL ASPECTS OF BLOOD TRANSFUSIONRaras P P100% (1)
- The Parts and Functions of Blood ComponentsDocument43 pagesThe Parts and Functions of Blood ComponentssatnamNo ratings yet
- Cme: Dengue Fever: by Nur ShafikaDocument47 pagesCme: Dengue Fever: by Nur ShafikaSyuk IdhamNo ratings yet
- Essential principles and complications of blood transfusionDocument27 pagesEssential principles and complications of blood transfusionisuhuNo ratings yet
- Blood Component TherapyDocument82 pagesBlood Component TherapyVivek GuptaNo ratings yet
- Dengue Short VersionDocument27 pagesDengue Short VersionDebbieWhiteNo ratings yet
- Dengue Spectrum FinalDocument43 pagesDengue Spectrum Finalshyam kumar MishraNo ratings yet
- Transfusion Process For NursesDocument31 pagesTransfusion Process For NursesShoheb ShaikhNo ratings yet
- 2 Dr. DjumhanaTI2014 - Tranfusi DarahDocument43 pages2 Dr. DjumhanaTI2014 - Tranfusi DarahMazaya EkawatiNo ratings yet
- Blood Grouping and BankingDocument41 pagesBlood Grouping and BankingChipego NyirendaNo ratings yet
- Blood ProductDocument35 pagesBlood Productrajan kumar100% (3)
- Transfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1Document33 pagesTransfusion Reaction and Coombs Test: Moderator:-Dr Sanjay Agrwal Presenter: - DR Pratima Singh PG Jr-1UmikaguptaNo ratings yet
- KeynoteDocument45 pagesKeynoteJim RohnNo ratings yet
- Serious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologyDocument65 pagesSerious Hazards of Transfusion: DR Kenneth S Charles MB - Bs (Uwi), FRCP (Uk), Frcpath (Uk) Senior Lecturer in HaematologySuneil R AlsNo ratings yet
- BLOOD TRANSFUSION NotesDocument7 pagesBLOOD TRANSFUSION NotesErl D. MelitanteNo ratings yet
- Pediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNDocument90 pagesPediatric Cardiology: Betsy Johnson, MSN, CPNP-PC Aya Rahav, MS, RN, CPNGelsey Gelsinator JianNo ratings yet
- Blood TransfusionDocument32 pagesBlood TransfusionDrPreeti Thakur ChouhanNo ratings yet
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Blood TransfusionDocument29 pagesBlood TransfusionNonu Kims100% (1)
- Updated Management of Dengue, ImrulDocument73 pagesUpdated Management of Dengue, ImrulFaheem Ul HasanNo ratings yet
- Paediatrics QuestionsDocument14 pagesPaediatrics QuestionsCedric KyekyeNo ratings yet
- JC - Group C Obstetrics and Gynaecology MCQsDocument5 pagesJC - Group C Obstetrics and Gynaecology MCQsCedric KyekyeNo ratings yet
- JC - Group B Obstetrics and Gynaecology MCQsDocument4 pagesJC - Group B Obstetrics and Gynaecology MCQsCedric KyekyeNo ratings yet
- Ong Cases Final-1Document49 pagesOng Cases Final-1Cedric KyekyeNo ratings yet
- Modern Family Planning MethodsDocument74 pagesModern Family Planning MethodsCedric KyekyeNo ratings yet
- Simply Put - ENT NOSE LECTURESDocument38 pagesSimply Put - ENT NOSE LECTURESCedric KyekyeNo ratings yet
- Simply Put - ENT EAR LECTURE NOTESDocument48 pagesSimply Put - ENT EAR LECTURE NOTESCedric KyekyeNo ratings yet
- 9966 Cons enDocument225 pages9966 Cons enOmz DonNo ratings yet
- Hazardous Material Management ProcedureDocument9 pagesHazardous Material Management ProcedureozerNo ratings yet
- 5 2 16Document8 pages5 2 16The University Daily KansanNo ratings yet
- Advance Endoscopy Assessment FormDocument2 pagesAdvance Endoscopy Assessment FormRomelia CampuzanoNo ratings yet
- Internship ReportDocument15 pagesInternship Reportpreethi balakrishnanNo ratings yet
- Medical Treatment of Aortic Stenosis: in DepthDocument19 pagesMedical Treatment of Aortic Stenosis: in DepthAlexandra NalgomNo ratings yet
- Assign No. 1 Module 6Document3 pagesAssign No. 1 Module 6Cindy Mae de la TorreNo ratings yet
- Stunting in Children Under FiveDocument11 pagesStunting in Children Under FiveIndah Tri AntikaNo ratings yet
- Đề Thi Thử Thptqg Môn Tiếng AnhDocument8 pagesĐề Thi Thử Thptqg Môn Tiếng AnhHổCápNo ratings yet
- Case Write Up - Dengue FeverDocument22 pagesCase Write Up - Dengue FevervijayaNo ratings yet
- Rare blistering skin condition linked to gluten intoleranceDocument2 pagesRare blistering skin condition linked to gluten intoleranceCharticha PatrisindryNo ratings yet
- THE AFFORDABLE ARTHRITIS & OSTEOPOROSIS CUREDocument18 pagesTHE AFFORDABLE ARTHRITIS & OSTEOPOROSIS CURENatalia NeliNo ratings yet
- Dien Bali Meeting 11Document5 pagesDien Bali Meeting 11Dien NingsihbaliNo ratings yet
- BS BuzzDocument9 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
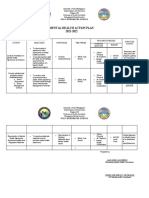
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- Msds Pipefit As Sds 2018 - 0Document5 pagesMsds Pipefit As Sds 2018 - 0solangelNo ratings yet
- Mental Health EssayDocument2 pagesMental Health EssayROHITNo ratings yet
- Doctors of KotaDocument14 pagesDoctors of Kotasanjay0% (1)
- MEng in HSE EngineeringDocument9 pagesMEng in HSE EngineeringZubair Khan100% (1)
- The Psychosocial Impact of Extreme Gaming On Indian Pubg Gamers: The Case of Pubg (Playerunknown'S Battlegrounds)Document8 pagesThe Psychosocial Impact of Extreme Gaming On Indian Pubg Gamers: The Case of Pubg (Playerunknown'S Battlegrounds)qhdpjqofoexsdfbsygNo ratings yet
- Atos CFSDocument22 pagesAtos CFSPaul SmithNo ratings yet
- Pdoc - Vivicit LeafletDocument1 pagePdoc - Vivicit Leafletahmedrijone2014No ratings yet
- How ergonomics improves employee performance and reduces costsDocument3 pagesHow ergonomics improves employee performance and reduces costsPradeep Dahiya100% (1)
- Communicable Disease 2Document5 pagesCommunicable Disease 2api-213445283No ratings yet
- Preterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)Document31 pagesPreterm and Posterm Birth: Oleh: DR Adi Setyawan Prianto SP - OG (K)ATIKAH NUR HAFIZHAHNo ratings yet
- JSA Basket TransferDocument3 pagesJSA Basket TransferCristina Rican100% (1)
- Birth asphyxia causes and neonatal resuscitationDocument20 pagesBirth asphyxia causes and neonatal resuscitationinne_fNo ratings yet
- World Vision Safe and Prosperous Urban Programming in BasecoDocument14 pagesWorld Vision Safe and Prosperous Urban Programming in BasecoTap TouchNo ratings yet
- Key Factors for Food Business SuccessDocument12 pagesKey Factors for Food Business SuccessOreoNo ratings yet
- Q4 Module 4 Answer Health 10Document3 pagesQ4 Module 4 Answer Health 10Brian MirandaNo ratings yet